Therapy for apraxia is direct and intense. Any task that involves motor planning is this way. Motor planning any skill, whether it be learning to shoot hoops, hit a tennis ball, or learning to speak when your etiology is motor planning (apraxia), instruction needs to be intense and involve a lot of repetitive practice.
I remember when I attended an intensive 4 day training, Dr. Ruth Stoeckel from Mayo clinic was asked how many repetitions SLP’s should be looking to get in therapy. She hesitated and expressed concern about giving a number. I didn’t understand her hesitation at the time. It was a simple question, how many repetitions should we be trying to get in therapy? We were all professionals. We all understood that this number would be in the ideal circumstance, and that many factors would decrease the number. Still, she was hesitant to give a number. She did finally say in the ideal circumstance, we are looking to get around 200 reps per session.
I now realize why Dr. Stoeckel was hesitant to throw out that number. It’s not only because it can only happen in the most ideal circumstances and we might frequently fall short. The main concern is that a number doesn’t take into account a child’s emotional health.
Let me say it again. Yes our goal is to get a lot of reps, but it doesn’t take into account a child’s emotional health!
I was talking to a student who is Ashlynn’s para right now and he is looking to earn his special education degree. He expressed concern that others seemed so much smarter than him and he was worried he wouldn’t be as good a teacher. He was the only person in Ashlynn’s life thus far who recognized her anxiety and nail picking and fixed it by buying her a rubber band ball. His professor actually admonished him for it. It just went to show his professor sitting at the university was completely out of touch with what was going on the field, and that was my point to this young man.
I have met brilliant SLP’s. Seriously brilliant. “C’s get degrees” does not apply in my field. I’m not trying to boast either, it just doesn’t happen. Graduate school for speech/language pathology is extremely competitive, and average GPA’s, AVERAGE, were 3.88 to 3.97 at the time I was trying to get into graduate school. That means a fair amount of current SLP’s held college level GPA’s that were 4.0.
It’s important to have the best of the best teaching our children to talk; however, a GPA can never account for what I would consider to be one of the most important qualities in an SLP. It’s a quality I can’t even succinctly put into one word, but it is by and far the most important. It is a therapist’s ability to read and then respond to the emotional health of their student or client. If we, in our quest to get 200 reps completely disregard any signs of emotional anxiety, distress, or defeat in the child; we have lost everything we had hoped to gain.
Let me say that again. If we sacrifice a child’s emotional health for the sake of getting in so many reps, we have lost EVERYTHING.
Speech therapy is predominately speech and language therapy, but the counseling aspect I believe is significantly underscored. My graduate program did include a class on counseling in speech therapy, but it was geared primarily to the adult population or for those who stutter. Our pediatric field recognizes now the importance of counseling in stuttering therapy, but there is very little information out there on counseling and our kids with not just apraxia, but also a phonological disorder, articulation disorder, or a language impairment.
What Dr. Stoeckel was trying to tell us in her hesitation of throwing out a number of reps we should be targeting, is that if we sacrifice their emotional health and our trust relationship with them for the sake of getting in a certain amount of reps, we have sacrificed everything.
I get sent videos from time to time asking for advice, and usually what I find striking is NOT the speech therapy that is being done, but the absolute blind eye turned to a child’s nonverbal signs of emotional distress. I remember watching one video and the child was enrolled in PROMPT therapy. The SLP was kind, competent, and skilled at what she was doing. What she never even once acknowledged though was that the child would constantly put his head in his hands when she asked him to repeat anything. Nothing was said. Nothing at all! Not, “It’s okay, I know this is hard, but you got this!” or “I know it’s so hard and I can see you are frustrated so let’s take a break.”
Nothing. Just, “Say it again, try again.”
It was all about reps and speech and reps and speech and reps and speech and reps and speech.
I’m here to tell you, if we aren’t addressing the head in the hands, the best and the smartest SLP in the world isn’t going to make progress. I told this student, if we aren’t addressing the nail picking that causes bleeding, the best and smartest SPED teacher in the world isn’t going to make progress.
Let’s go back to motor planning though, since the research is telling us that is the most effective form of treatment for apraxia. If we liken it to another motor skill like basketball, is the job of a coach JUST to teach the kid the right technique and the right form to shoot a basket? Or, is the job a coach to also encourage, foster, and nourish their confidence as well? In that analogy, it seems obvious; yet with speech therapy we still don’t seem to be there yet.
A final example comes from a newer client of mine. Completely nonverbal at the age of 7, her school SLP, who is amazing, risked her job to recommend private therapy. After three months, she was making progress, but much, much slower then I wanted. She had major avoidance behaviors and if she were asked to repeat anything again she would point to something else, pretend her finger hurt, or try to get off topic. The avoidance behaviors decreased the more she developed trust and had success, but I still felt like I was missing something.
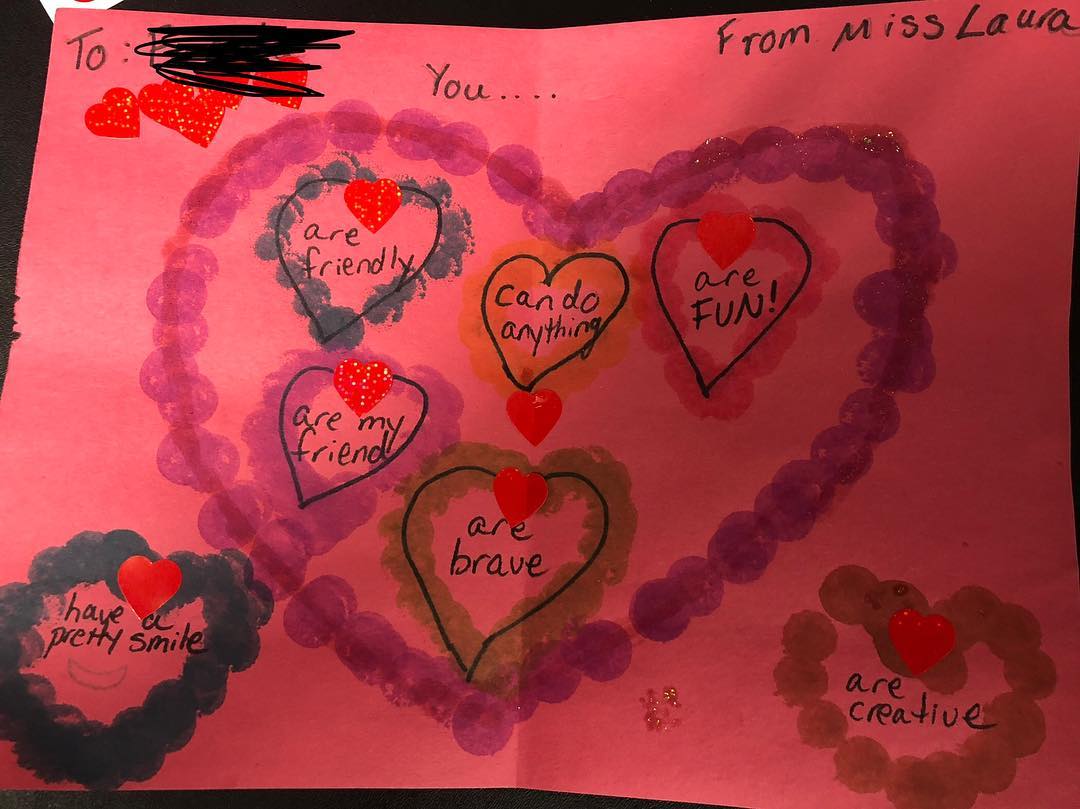
Since Valentine’s day was coming up, I decided we would take a break from speech and do something fun. Make Valentine’s. I still embedded a few target words in the activity, but for the most part, the focus was on the Valentine. She made one and I made one. When I showed her mine, I read all the things I wrote about to her. I stressed that she was brave and could do hard things. Her brown eyes searched my face, wanting to believe me. When I read she was creative, she proudly pointed to the Valentine she had made, and I nodded in affirmation. After the session, I had her mom come in and read it. She beamed as her mom read the words on the page. Before she left I looked her in the eye again and told her she was brave and could do hard things. This time, though her eyes still searched my face, she nodded her head.
The next day her school SLP sent me a video. She had a breakthrough and said two new words and her confidence was through the roof. We both decided taking time to address her emotional health was going to be just as critical to her speech progress as were the principles of motor learning.
My message today is this. You can have the smartest, most competent, adept and amazing SLP in the world; but if they aren’t addressing the head in the hands, the avoidance behaviors, or a child’s emotional heath; they are sacrificing EVERYTHING. In our quest to provide good therapy for apraxia, we keep in mind the principles of motor learning, but ALSO what it means to be a child’s coach and champion. That might mean some sessions we elicit 0 reps, but what we gain in trust is immeasurable.
Be the therapist who is looking to give good therapy, but who first and foremost is always looking for and then addresses the head in the hands. Your kids will thank you.