I only realized after being a part of the special needs community that school SLP’s have a bad rap. Like a really, REALLY, REALLY bad rap.
I’m preparing a talk next month for Colorado school SLP’s, and every time I prepare a talk for this demographic, I have to tell you they have a special place in my heart. No, it’s not just because I started as one and work as one part time, but it’s because I have literally worked under, with, and around many, many, MANY of them. I have worked with so many of them, and I can tell you they are a jack of all trades. They are the EXPERT in eclectic, and may be the ONLY person in the school who understand in depthly just how a student’s unique communication challenges actually affect them in school.
In the schools, you don’t have the option to specialize. Kids from every disability show up on your caseload and you are expected to be the expert. It might be hard to understand as a parent, but there are soooo many different disabilities and speech and language disorders, and a parent (rightly so) expects the SLP to do right and best for their baby.
Every single SLP I know and have met has a desire in their heart to help children. Please, let that sink in.
When I took Ashlynn to her first private SLP who had never worked in the schools she was asking me about qualification. She asserted that she could never be a school SLP because she felt it was unethical to not qualify students who clearly had some sort of speech or language problem. I had a hard time refuting her. Aside from saying qualification is different in the private versus educational sector, I really had no excuse. I know that funding is limited in the public sector so that obviously plays a part in qualification. I also know if every SLP took her stance, than NO kids would be serviced in the public schools, and is that really what we are going for?
Public school SLP’s have caseloads that are probably double if not more of the private SLP.
Where the private SLP can see kids 1:1, school SLP’s rarely have that luxury. With weekly caseload averages around 45 to 55 and some maxing out at 90 (Yes 90 people I’ve seen it), even the most skilled SLP will not be able to do what a private SLP can do 1:1 for 45 minutes (though they will kill themselves trying).
The result? Parents become outraged at the lack of progress or progress they feel the child should be making. They surmise the school SLP just isn’t as good as the private SLP and they become disillusioned and write them off. They post memes about preparing for battle when going into an IEP meeting!  This honestly breaks my heart. I feel bad for the parent who feels the SLP doesn’t care, and I feel bad for the SLP who is trying to manage an unmanageable caseload, writing IEP’s at night,
This honestly breaks my heart. I feel bad for the parent who feels the SLP doesn’t care, and I feel bad for the SLP who is trying to manage an unmanageable caseload, writing IEP’s at night, or staying up until 2 Am (true story from an SLP I just talked to last week) to write a lesson plan, only to be ravaged by a parent unsatisfied with the results.
or staying up until 2 Am (true story from an SLP I just talked to last week) to write a lesson plan, only to be ravaged by a parent unsatisfied with the results.
I’m not sure if everyone is aware of this, but ANY SLP in ANY setting is as qualified as the next SLP by basic certification standards. What does that mean? That means, as long as an SLP received their masters degree and the Certificate of Clinical Competence (CCC) through ASHA they can work anywhere. So that means, your school SLP can apply for a job at Children’s Hospital right now and probably get hired tomorrow (because in case you didn’t know there is an SLP shortage as well). For some reason though, there is this perception that the school SLP just isn’t as good as the private SLP. If it’s true, it probably has MORE to do with caseload and workload size than it actually has to do with the qualification of the SLP.
I get calls and emails all the time from concerned school SLP’s desperate to meet the needs of their kids with apraxia but not knowing how. They want to see the kid more, or see the child 1:1, but their caseload simply does not allow for it. They cannot add more hours to the day, yet they still call, or write and wonder if there is something they have not yet thought of. Oh, and here’s a dirty secret. Listen close.
Are you listening because this is VERY important.
If an SLP feels in their heart a child needs private, supplemental speech services, they CANNOT say it. People, they CANNOT tell you this. Why? Well, their license and job is on the line. In most cases, school SLP’s are told not to recommend any sort of outside therapy. Why do you ask? Why?
I’ll tell you. If a school SLP recommends outside services, the parent can sue the district and win, and potentially disbar an SLP from ever practicing again. Are you asking why again? I’ll tell you. If a school SLP recommends outside services, they are essentially saying that the child can not benefit or make progress from the therapies provided by the school, and the school is required by law to show progress. If the SLP recommends outside service thereby saying the school is inadequate, the school gets worried or they will get sued for not providing adequate services and the SLP potentially fired.
Would you take that risk?
I’m not saying unilaterally every school district would do this, I’m just saying, school SLP’s are told this is a possibility, and so they would find it best not to recommend outside services.
You need to know this as a parent of a child with any disability. Some SLP’s will risk their professional license and recommend this to you. Let me tell you though what they are risking. They are risking 4 years of a bachelor degree, 2 years of a masters degree, 1 year of a clinical fellowship, and the usually 3 years of probationary status as a teacher. That is an entire decade of work and dedication to a profession they love and believe in. Would you take the risk then to recommend a parent pursue outside therapy? This is where they are at! It is truly a catch 22.
If you are upset about your school services, you probably have every right to be! I was VERY unhappy with Ashlynn’s preschool, in-class only, speech/language services. However, it is important to place the blame on the right entity and in most cases I can assure you it is NOT on the school SLP’s shoulders. In Colorado, the Colorado Department of Education mandated an inclusion model only of special education services in preschool thus making it extremely difficult for any school SLP to pull a student out into a 1:1 session.
My message today is this: School SLP’s are some of the most phenomenal group of people I ever have the honor to speak with or to. They do not get the option to specialize, and so they pursue advanced training and expertise in every disability that may affect communication: from Apraxia to Angelman’s Syndrome, from Developmental Delay to Down Syndrome, from Cerebral Palsy to Stuttering, from Language Impairment to Nonverbal Learning Disability, from Assistive Technology to Autism, from Auditory Processing Disorder to Articulation Disorder, school SLP’s will see it all and be expected to rise to the challenge. They cannot “refer out” or “discharge for lack of progress” as an can be done in private speech. No, the school SLP is expected to figure it out regardless of the lack of resources, lack of funding, or lack of time.
They will be faced with limited or no space, they will be strapped with high caseloads, and criticized by parents; yet they will persist and pursue only becoming better for it, because of their love for the children and the profession. I personally have witnessed it time, and time, and time again!
I can tell you firsthand, getting into graduate school for speech/language pathology is VERY difficult. It is highly competitive, and here in Colorado, the average COLLEGE GPA was a minimum of 3.87 when I applied. I found this graphic from 2011 but I can tell you things have not changed much. There is a HUGE gap between the number of applicants and the number of people selected. 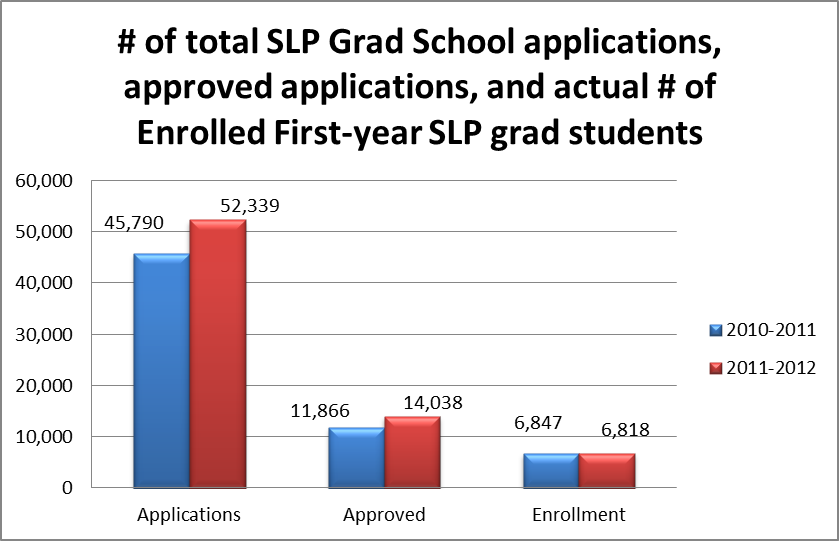
The disparity should be striking, and please remember that MANY of these applicants will be YOUR school based SLP. If you have the mentality that “C’s get degrees” and you are certain your school based SLP fits the latter, let me correct you. NO average C students make it to graduate school in the first place for speech/language pathology.
Truth
For my final thoughts I wish not to be adversarial. I hope that this article has persuaded you, a parent OR SLP, to reach out to the other side and bring about the change you wish to see. I have the unique perspective of being on both sides, and as such, I have the utmost RESPECT and LOVE for both sides. I truly wish for there to be a conduit of communication, and not a ridge of animosity and distrust; and at the the forefront, I wish to impart a spirit of solidarity between my professional and special needs relationships.
To read more from SLPMommyofApraxia follow her on facebook, pinterest, or twitter.