Hi readers! Not only another year, but another decade is coming to a close! My daughter Ashlynn was born in 2009, and it’s astounding all of the changes that set off in my life throughout the past ten years! This past decade was one of joy as a I built my family, but also sorrow facing numerous challenges with Ashlynn.
I have faith though that this next decade will be one of overcoming! I know ten years from now I’m going to be writing another success and triumph story, much like I did in the book I published this year called “Overcoming Apraxia.” I also want this next decade to be one of exponential growth in apraxia awareness and information so all children have the access to the best therapy.
On my facebook page SLP Mommy of Apraxia, every Sunday I post a kids being kids moment. The idea was to show the world that kids with apraxia or other invisible disabilities enjoy doing the same things as neurotypical kids. One day, a mom remarked she felt bad she didn’t have the money to give her kid all the experiences other parents seemed to be giving their children.
I told her that the gift of her presence was the best gift of all.
This year I lost my grandmother. She was honestly one of the most positive and pivotal influences on my life during my formative years and then throughout the rest of my life. What I remember about her was not the presents she bought. I mean I do remember that she was there for every birthday and Christmas and that she always gave me presents. That’s not what left the impression though.
I remember when I was with my grandma I was the most important person in the Universe. What I DO remember is helping her make her bed in her room with the violet walls. I remember helping her hang up the wash outside. All of these things were “chores” at my house but anything was fun with my grandma. I remember she would play card games with me and she would cook me breakfast. I remember she would take me with her when running errands or to the pool where she did her aqua exercise. The gift of my grandma was in the mundane, because…
Her presence was the greatest gift.
She will be dearly missed, but I feel so blessed to have had her in my life. I feel so blessed to have learned at such an early age thanks to her the words that Maya Angelou so eloquently once said,
I’ve learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.
To put it simply. I felt loved because she was present, and she was present with me and THAT is truly the best gift we can give.
This holiday season, whether you have abundance or modest means or somewhere in between, never forget that YOU being present with the ones you love is the greatest present of them all.
I recently posted a quote from my book Overcoming Apraxia that was met with a lot of questions. The first question was from SLP’s asking about the additional trainings and resources I would recommend. You can read about that here. The second question came from parents wondering what questions to ask? I’ve created a (not exhaustive) list of questions to ask a potential SLP about their knowledge and experience treating childhood apraxia of speech.
As I was writing them, I thought, though this list is a great starting list for parents, this is ALSO a great list for SLP’s to ask themselves when evaluating whether they are actually an expert in it! Self reflection is always good, right?”
Okay so here we go! My top ten questions for speech-language pathologists!
How comfortable do you feel treating childhood apraxia of speech?
What other questions would you ask? Find me on social media under the handle SLP Mommy of Apraxia and let me know!
Laura Smith, M.A. CCC-SLP is a 2014 graduate of Apraxia Kids Boot Camp, has completed the PROMPT Level 1 training, and the Kaufman Speech to Language Protocol (K-SLP). She is the author of Overcoming Apraxia and has lectured throughout the United States on CAS and related issues. Currently, Laura is a practicing SLP specializing in apraxia at her clinic A Mile High Speech Therapy in Aurora, Colorado.
I recently posted a quote from my book Overcoming Apraxia on social media that garnered quite a bit of attention. It wasn’t to criticize or disparage SLP’s. It’s just a fact many of us speech-language pathologists, (myself included) didn’t get adequate training in graduate school on how to treat apraxia. I had maybe 15 loose leaf pages on it, and that wasn’t about treatment.
Many SLP’s asked what trainings I would recommend and many parents asked what questions they should ask. I’ve compiled a list of trainings and resources on childhood apraxia of speech for speech-language pathologists.
SLP training and resources
There are numerous online free trainings for apraxia, believe it or not.
Currently Edythe Strand has a free course on DTTC (dynamic temporal tactile cueing) that gives you CEU’s through the University of Texas at Dallas found at Child Apraxia Treatment.
Apraxia-Kids.org offers on demand videos that can be accessed through a yearly subscription fee that is relatively cheap (around $90 for the entire year).
ASHA.org has a recently updated practice portal on CAS.
A newer and AWESOME book targeted for parents and early intervention professionals is “Let’s Get Talking,” by Mehreen Kakwan. It explains direct therapy tips to use when a child has suspected motor planning difficulties including visual and verbal cueing ideas.
*Both DTTC and ReST have the current highest evidence base in the research on apraxia*
Fellow speechies, here’s the deal. Yes we come out of graduate school with a wealth of knowledge, and yes, the Certificate of Clinical Competence behind our name makes us qualified to treat speech/language disorders; however, the field is VAST. We should not apologize or feel bad about not being an “expert” in every speech and language disorder from birth to geriatrics.
However we DO have a responsiblity to be honest with parents, clients, and families about our level of expertise in a given area, and whenever possible, try to gain additional training and expertise in that area if we are lacking.
Laura Smith, M.A. CCC-SLP is a 2014 graduate of Apraxia Kids Boot Camp, has completed the PROMPT Level 1 training, and the Kaufman Speech to Language Protocol (K-SLP). She is the author of Overcoming Apraxia and has lectured throughout the United States on CAS and related issues. Currently, Laura is a practicing SLP specializing in apraxia at her clinic A Mile High Speech Therapy in Aurora, Colorado.
I’m so excited to have some of the two largest apraxia social media influencers with me today to talk about what it is like to be “Adulting with Apraxia.” Mikey Akers from Mikey’s Wish and Jordan LeVan from Fighting for my Voice are both young men living with verbal apraxia. In the UK, verbal apraxia is known as verbal dyspraxia.
Jordan and Mikey were talking one day about various issues that affect them in their adult life and wanted to write a piece together. I think it’s such an important topic, as apraxia cannot be cured and many adults live with residual effects and experience difficulties in which others might not even be aware. For example, Jordan once was talking about his struggle to find a job. It took him around a year just to find gainful employment. Today our hope is to go beyond the misconception that apraxia is just a speech disorder of childhood and talk about what it’s like, “adulting with apraxia.”
Let’s get to it!
Let’s begin by talking about some of the residual effects both of you deal with today. Let’s start with word finding. Mikey, you have said before that your word finding issues make it look like a lack of confidence when that is not the case at all. Jordan, you have described moments when the word is in your head but it simply will not come out of your mouth. Will you both elaborate on this?
Jordan: Essentially, my speech disorder is known for the following: your brain having trouble sending your mouth signals, for accurate movements of speech. So, at times, I’ll know the exact word I want to say; however, my brain simply didn’t send that signal to my mouth. More occasionally, words are harder to get out, as well as words with multiple syllables. I also do struggle vocal fluency, so my voice is essentially monotone a lot of the times. I have to be putting effort in directly in the given situation to create those various tones people display in their voice when they’re happy, excited, and sad.
Mikey: Word finding is one of my biggest struggles now that I have found a voice. It is what holds me back, where my speech is concerned. It is what stops me from engaging in conversations with people that I don’t know. It affects my confidence and self esteem and it is the main cause of the anxiety that I have surrounding my speech. At times I stop mid sentence because the word I need isn’t there. This makes my speech disjointed as I pause, frantically looking for the word I need or one that means something similar. Everyone’s had those “the word’s on the tip of my tongue” moments, right? Well it’s like that but it’s every time that i want to talk. As far as talking is concerned I lack confidence but I am confident in every other area of my life.
2. Mikey you have been open about your anxiety. Does this exacerbate your word finding difficulties or is this a separate issue altogether? Jordan, do you struggle with anxiety as well and if so how?
Jordan: I was diagnosed with Generalized Anxiety Disorder, as well as Anxiety due to chronic health issue known as Apraxia. I first received help whenever I was twenty years old. My anxiety related to Apraxia relates to thoughts about, “What are they gonna think about my speech?” “Does she/he/they think I’m “dumb” if I can’t get a word out?” Naturally, not being able to get words out is so anxiety provoking. You go in for the word, but it just hesitated to come out from your lips. Your face feels tense now, your palms are sweaty now, and you’re trying to catch your breath back from having trouble over trying to get that word out. You would feel one of the things I just mentioned most likely just from occasionally not getting a word out right the first time. I’ve learned how to cope with my Anxiety with therapy. Therapy is now becoming socially accepted in our generation, as it should be. It’s the one resource that’s made me okay with essentially owning my voice.
Mikey: It’s a vicious cycle. I have huge anxiety where my speech is concerned, this stems from the years of people not understanding what it was that I was trying to say. I know that I now have a voice that others can understand but I worry when I try to talk to someone who doesn’t understand my difficulties that my words won’t come. I worry that they won’t be able to understand what it is that I am trying to say or that they will think that I am stupid for being an adult and not being able to speak properly. Then because I am worrying so much and feel anxious the words really won’t come, no matter how hard I try to force them out, even though I know in my mind what I want to say. Frustrating is an understatement but I am determined to keep fighting to overcome this debilitating anxiety.
3. It has been reported that many individuals with apraxia have difficulty with modulating vocal volume. This can be where the person is speaking too softly and cannot be heard over ambient background noise, or conversely may be speaking too loudly and not realize it. Do either of the above scenarios happen to you and if so how?
Jordan: I speak to softly. This happens typically in my day to day life when a person will tell me they can’t hear me. Even when I’m trying my best to speak louder. I can speak louder, but it often comes out louder than I would like it too. People have even been shocked at me yelling. My own mom said to my own speech therapist, “So, he can yell?” A little funny story. Scenarios of this currently happen to me in classroom settings, work, and on the phone.
Mikey: When I was younger I had a very loud, high pitched voice when I was at home and felt at ease with those around me. I never realised just how loud I was but I was constantly being told not to shout. When I was at school or around unfamiliar people I would choose not to speak. Now I have a normal level of speech when I feel comfortable but the minute I am out and about amongst people I don’t know my voice reduces to little more than a whisper. My mum always asks me why I am whispering as she can’t hear me, I don’t even realise that I am doing it.
4. Both of you have mentioned that it may take you slower than some people to process language. In the apraxia community at large we have a saying, “I know more than I say, I think more than I say, I notice more than you realize.” Do either of you relate to this saying?
Jordan: I do with some of the following, I don’t believe so much with the “…I notice more than you realize.” Because if somebody makes a misconception about my speech, I’ll directly inform them. I usually will express my thoughts in given situations, however, I won’t expand further into the conversation because of difficulty. I can feel mental exhaustion from speaking, and sometimes I simply need a break to recharge. I’ve been able to expand on conversations even further now in my adult life with incorporating hand movements and hand gestures.
Mikey: I can definitely relate to this. People assume that because I struggle to verbally express my thoughts and feelings that I have no opinion on subjects that are being discussed, which just isn’t the case. This happens more when I am in a larger group as the conversation flows so quickly that by the time I have processed the beginning of the discussion and have found the words to reply the conversation has usually moved on to the next topic. If people just slowed down the conversation they would realise just what I ‘know’, ‘think’ and ‘realise’.
5. With this flurry of struggles hiding beneath the surface, how does this present in social situations? Work situations?
Jordan: I believe in social situations a majority of people assume I’m either nervous or shy. I get told quite often that I am so shy. In reality, I’m not really that shy. I believe everybody can be to a certain extent. It may also look like in work situations that I don’t know what I’m doing, since my speaking is at a slower pace than others with word difficulty. Others have came up to me and asked, “Have you got that ‘good good’?” I asked, “No, why do you ask that?” He asked “Aren’t you high?” I said “No, what would make you think that?” Then he didn’t answer, and he handed me my tray of food. Other assumptions about me being under the influence of drugs has also happened with police officers and doctors. We will get to that part soon.
Mikey: In social situations, with friends, I am very confident and outgoing but it takes a long time to reach this level of comfort. I put up protective walls and only those with the patience to keep chipping away and get to know me get to meet the real me. If it’s a social event where I don’t know many of the people attending then I probably come across as extremely quiet and shy. Maybe even being mistaken as rude, although this really isn’t the case.
6. It has been reported that individuals with apraxia struggle with foreign language in highschool. Did either of you and if so what accommodations were made?
Jordan: I did struggle with foreign language, since it does rely on pronouncing the words correctly. Because of my speech disorder, grading based on pronunciation isn’t practical. In high school, they essentially counted the credits without participation in class. In college, I’m actually exempted from foreign language classes. The accommodation board wants to make sure my speech isn’t critiqued by professors.
Mikey: I never studied a foreign language in school. I was so far behind in all my other lessons, due to my severe struggles with literacy, that I had extra English lessons when everyone else was learning French. Everyone thought that this would be more beneficial to me than trying to learn a foreign language.
7. Have you found people in the general public to still be rude or intolerant of your speech differences? If so how?
Jordan: Yes. I’ve had people in customer service tell me if I don’t speak so slow they’d take my order. I’ve had doctors say “Well, Verbal Apraxia seems to be a speech issue. This doesn’t affect your reading or anything else.” Meanwhile I didn’t grasp reading until I was nine years old. I’ve had people try to rush my speaking, laugh at me, and say “Any day now buddy.” The general public wants fast and immediate speech responses. It’s because we live in a world where we are constantly going. My general speaking may take some more time. It doesn’t make it a bad thing, everybody’s voice is different. It just seems like if you don’t fit the “norm” you can be considered an inconvenience.
Mikey: I have very rarely experienced any rudeness or intolerance because of my speech issues. I have only had 1 incident when a bus driver asked why I was being stupid as he didn’t understand me and this situation was very quickly dealt with, ending in an apology and another person being educated in Verbal Dyspraxia. I have had some people ask about my speech as they are genuinely interested in learning more about my diagnosis. When we get into a conversation with people that we meet in social situations (as a family) we find out that they had just assumed that I was hard of hearing, like my dad. I am still very much in the safety net of education though as I haven’t ventured out into, the slightly less forgiving, working world yet.
8. Have either of you had a run in with law enforcement and were mistaken for being under the influence of alcohol or drugs? If so, how was it handled?
Jordan: I was pulling out of a gas station one night, and I forgot to immediately turn on my headlights until I pulled out. The police officer pulled me over, and I asked why was I pulled over? He said it was because I didn’t turn on my headlights until after. I responded with “Oh yeah, I didn’t realize I didn’t have them on until after I left. I’m sorry.” He then asked me, “Are you drunk?” I said, “No sir.” He then asked, “Are you high then?” I said, “No sir?” He then asked me if I’d ever drank, ever smoked, and continually asked these two questions five times over each. Each time he would re-ask the question, in this ten question trivia game of his, my speech would become more disorganized, because of the pressure of the situation. He was smirking. I’m sure in his mind the assumption was “When people lie, their speech becomes more disorganized.” He then let me go after his game was over.
Mikey: No, thankfully I have never had a run in with the law.
9. Person first language (I’m a person with apraxia versus I’m apraxic/dyspraxic) is a hot button topic. It used to be, person first language was the law of the land until individuals with autism started saying they wanted to be referred to as autistic. Do either of you have a preference?
Jordan: I don’t really have a preference. I feel like the message that comes with “I’m an individual who has Apraxia” serves a reminder to me, that I am more than my Apraxia. However, I know this even if this is said or not. I feel like in our day and age, more people are owning what makes them who they are. I feel like saying I’m apraxic, doesn’t take away that at core, I’m a human being.
Mikey: I have no preference, it’s not something that bothers me. I am a person who lives with verbal dyspraxia/apraxia and in my mind that is not going to change whatever term someone else chooses to use.
10. What final message do you have for others who may be “adulting with apraxia” in the shadows?
Jordan: Apraxia is a tricky, still very poorly understood, neurological based condition that isn’t outgrown. I’m sorry if the term, Childhood Apraxia of Speech, made you also believe as a kid, that this is only a condition present in childhood. You didn’t do anything wrong, so please don’t ever blame your child self. Have compassion for yourself and how far you’ve come. Self comparing yourself to a person without your condition is a toxic. Would you ever compare an individual in a wheelchair with an able bodied person? If you would like to go back to speech therapy, it isn’t just for kids. If you’re ever feeling any negative mental health side effects from living with Verbal Apraxia, reach out for help. I know these resources aren’t always accessible for everybody, but at least talk with someone. Know that you aren’t alone. I hope one day I can hear your story. I want to actually. Literally message me, I’ll be cheering you on.
Mikey: Don’t be ashamed of your diagnosis, talk to others, let your employers know which areas you struggle with. Be honest about your feelings with those around you and more importantly be honest with yourself. The term Childhood Apraxia of Speech is misleading, this diagnosis doesn’t just disappear when you become an adult. You really are not alone, there are many of us living with verbal dyspraxia/apraxia as adults. If anyone ever needs to talk, I am always ready to listen.
You two are amazing and as a mother to a child with apraxia but also as a speech/language pathologist I can’t thank you enough for your bravery, insights, transparency, hope, honesty and encouragment to those living with your diagnosis. I can’t wait to see what the future has in store for you both!
SLP Mommy of Apraxia is a website dedicated to disseminating research, information, and stories about Childhood Apraxia of Speech (aka verbal apraxia, aka verbal dyspraxia). Follow us on Facebook, Instagram, YouTube
About a year ago, NPR published an excellent article discussing how the 30 million word gap needs reframing. The idea of the word gap started with two developmental psychologists Betty Hart and Todd Risley in the 1960’s. I first learned about the study as an undergraduate student in my speech and language development classes. I remember as a naive student learning that parents who didn’t talk to their children as much caused children to have a depressed vocabulary. I didn’t realize how dangerous this type of lesson was, as not only was the study itself fraught with racial bias, but it essentially “blames” parents when a child has a reduced vocabulary. I was taught this in a class where I was studying to be a speech/language pathologist who would help kids with legit language disorders. Does one see the problem? I was being taught about language disorders and simultaneously was learning about a study that said children have reduced vocabularies because their parents didn’t talk to them.
I only realized after I had a child with a communication disorder, just how judgemental professionals can be. This is in light of me being a white, graduate level speech/language pathologist. I started to realize how well-intentioned studies like the 30 million word gap end up blaming parents instead of doing what they say they intend to do, which is to help close the gap.
Now a new research article has caught fire and is making the rounds. Instead of blaming parents for not talking to their children, it’s blaming parents for not reading to their children. Today I invited two professionals with me to dissect the article and review it from our varying perspectives. I (Laura Smith, Speech/Language Pathologist) will be commenting from the view of monolingual children with Developmental Language Disorders (DLD). Teresa Gillespie (Bilingual Speech-Language Pathologist) will be commenting on the perspective of (culturally and linguistically diverse variables to consider for bilingual speech-language assessment and intervention), and Kara Viesca (Associate Professor of Teaching, Learning and Teacher Education) will be commenting from the perspective of multilingual language development. Hello ladies! Thank you so much for being here! I can’t wait to break down this very important topic!
1. What are the positives to a study like this?
Kara: We do know the positive benefits of reading with children and this study appears to be seeking to underscore those benefits and wanting to inspire more reading with children.
Laura: I can’t find any.
Teresa: When I look at the landmark study by Betty Hart and Todd Risley regarding the “word gap,” I remind myself that the purpose of their study was to explore the differences in language development and later academic achievement between children from lower socioeconomic levels and those from higher socioeconomic levels. They sought to understand the causes of these differences. From this perspective, I think that a positive in studies about “word gap,” “talk gap,” or “language gap,” is that researchers continue to search for and explore the reasons for the differences in the language development and educational performance of children from lower versus higher socioeconomic levels.
2. What are the dangers in a study like this?
Kara: We live in a very diverse society with a lot of complexity in the differences across home life based on cultural and linguistic practices. A study like this is can be used to promote the cultural and linguistic norms of one cultural group (White, middle-class, monolingual English speaking) over those of another and in the end blame parents and families for students performing in particular ways in school.
Laura: As a Speech/Language Pathologist (SLP) and mother to a child with a language disorder, simply reading a book will not be enough to ever acquire the vocabulary or language naturally in kids with DLD. These children require explicit and direct instruction and engagement with a book. I get concerned when I see studies like this because SLP’s are quick to spread the “positive” message on the benefits of reading and how many more words a child is exposed to when being read to; however, this can flirt with the dangerous idea that children who continue to struggle with language or have a low vocabulary have it because they were not read to enough. Instead, there is a possibility that the child has a legitimate language disorder.
Teresa: As a Bilingual Spanish/English-speaking Speech-Language Pathologist, I received specialized training on the different culturally and linguistically diverse factors to consider in bilingual speech-language assessment and intervention practices, including during the review of research study results that may affect those practices. When I look at the results of the original study by Hart and Risley, I ask myself how they apply to the population of individuals whom I serve. I work with bilingual Spanish/English-speaking Kindergarten – 12th grade students with identified speech-language difficulties in both Spanish and English. I can’t apply the results of the Hart and Risley study to the population I serve because they did not include bilingual Spanish/English-speaking individuals in their study. In fact, to my knowledge, there currently aren’t any published “word gap” research studies in the United States that include bilingual speakers of English and languages other than English. It would be inappropriate for me to apply the results of any “word gap” study to my bilingual speech-language pathology practices that consider vocabulary and language development in only the English language, which is a second, and sometimes a third, language for the population I serve. Any professionals, such as General Classroom Teachers, Special Education Teachers, Reading Interventionists, Speech-Language Pathologists, etc., who work with bilingual speakers of English and languages other than English need to consider the vocabulary and language development in English as well as the languages other than English in order for their services or assessment/intervention practices to be sound. This is true for not only bilingual speakers, but also for trilingual and multilingual speakers. The results of numerous research studies in the professional fields of psychology, speech-language pathology, linguistics, etc., indicate that considering the vocabulary and language development in only the English language for bilingual speakers underestimates their overall language abilities. When the vocabulary and language development of bilingual speakers focuses only on the English language, then the application of the results of the “word gap” studies becomes about English language proficiency and not true language abilities.
3. What biases are present?
Kara: We have to be honest about the reality that biases are always present in all studies as well as in our educational practices and policies. One of the typical biases we have is based on what we consider “normal” — this is how we create and perpetuate ideas about gaps. If we consider it “normal” for children to have the linguistic practices of White, middle-class, monolingual English speaking families, than students who come from different backgrounds will often appear to have a “gap.” If the norm was altered to mirror the linguistic and cultural practices of students from Latinx, bilingual English/Spanish families from the working class, then the students who currently appear to not have a gap, would appear to have one. In education around language, we hold English monolingualism and White middle-class culture as the norm for which all students should strive–a clear, pervasive and ongoing bias that continually positions certain students to have “gaps.” This study holds this same bias, assuming a particular norm is what all students and families should be aiming for that doesn’t account for legitimate, helpful and valuable cultural and linguistic variations that occur across families and cultural groups.
Laura: In terms of children with language/learning disabilities, they are not even addressed in the study. The article didn’t prove anything except to show that kids who are read to are exposed to more vocabulary and then cite other (biased) studies showing how exposure to more vocabulary is linked to the later vocabulary trajectories.
It’s important to mention studies showing how children with DLD have difficulty picking up vocabulary implicitly and need explicit instruction, before making conclusions that their vocabulary exposure contributed to their acquisition and retention.
Teresa: One of the biases is that children from lower socioeconomic levels come from homes where they receive less vocabulary and language development experience. This is not the case. The results of a recent study by Douglas Sperry, Linda Sperry, and Peggy Miller indicated that children with fewer vocabulary words and low language development skills did not all come from homes with lower socioeconomic levels or less vocabulary and language development experience. There was a wide variation in home language experience among all socioeconomic levels.
Another bias is that children have the same kind of language enrichment experience at home regardless of cultural and linguistic background. This is not true. Different languages and cultures provide different language enrichment experiences at home. Even different dialects and subcultures provide different language enrichment experiences at home. There can be oral language experiences that do not include parents reading books to their children. Instead, the parents tell and retell folktales or sing ballads that share the knowledge, ideas, and beliefs of their culture to their children. In the absence of factors that negatively impact language development, these children do not experience any less academic achievement than those children whose parents read to them from books. There can be language experiences that do not include parents providing comments or asking questions about what their children are doing, how they are doing it, etc. Again, in the absence of factors that negatively impact language development, these children do not experience any less academic achievement than those children whose parents provided comments or asked questions about their children’s various activities.
A third bias is that children who have adequate vocabulary skills and “typical” language development in English will experience academic achievement. Again, this is not the case. There are children who exhibit adequate vocabulary skills and “typical” language development in English who do not experience academic achievement. Also, provided with the appropriate supports, both in the home and school environments, children exposed to a language or languages other than English, as well as English, can and do experience academic achievement. To focus on vocabulary and language development in only the English language for bilingual, trilingual, or multilingual speakers is to diminish the benefits of bilingualism/multilingualism, and possibly cause members of other cultures to feel less important or respected.
4. What suggestions do you have for supporting children’s linguistic development?
Kara: My area of focus is in multilingual language development, so from that perspective I suggest doing as much as possible with language, particularly in authentic ways for meaningful communicative purposes. Children who live multilingual lives have developed strong communication abilities that respond to the communities and people they seek to communicate with. Too often at school, we don’t acknowledge this and focus on “gaps.” I’ve even sat at the table with a state commissioner of education who said, “These kids are showing up to school with no language.” I quickly called him out on this statement, because the kids he was talking about (and why I was at the table) are bilingual/multilingual students who, barring disabilities, have expansive language skills. They just might not be the language skills we have set as the norm or value in our schooling practices. In fact, this practice of constantly comparing multilingual students to their monolingual peers and identifying “gaps” creates an ongoing context of deficit thinking towards multilingual students. I resist focusing on gaps to the extent we do in education as I think we get too bogged down in “needs” and “gaps” and don’t work with students from a position of their strengths and learning assets. A child who did not have the traditional White, middle-class, monolingual English speaking literacy experience before they came to Kindergarten did have a lot of important linguistic and cultural experiences that offer strengths to that learner in school. We just have to learn to see those strengths, embrace them and work with students to grow them.
Laura: From the perspective of children with DLD, linguistic development is enhanced through therapy and direct and explicit instruction. No amount of just talking to or reading to the child with DLD is going to help them overcome a language disorder. That doesn’t mean talking to and reading to children with language disorders doesn’t “help” but it’s not the entire piece of the puzzle. Parents and professionals can change the way in which they read and talk to the child and employ strategies that help the child with DLD process and use language effectively, but this is done through the skilled care and recommendations by the speech/language pathologist. In sum SPEECH THERAPY is the most effective way to treat language disorders and build vocabulary.
Teresa: For me, the most important suggestion for professionals in the United States who work to increase the vocabulary and language development of bilingual/multilingual speakers is to encourage the continued understanding and use of the native or home language(s) while fostering the acquisition of English. English language development can successfully occur in an “additive bilingual” environment. An “additive bilingual” environment not only promotes the continued learning of the native or home language(s) while learning English, but also preserves the cultural identity or identities of the speaker, which leads to a feeling of being valued.
The most important suggestions for parents of bilingual/multilingual speakers of English and a language or languages other than English are to maintain the native language(s) in the home environment, and become as familiar as possible with the academic expectations for each grade that your child attends. It is also important to become as familiar as possible with the academic resources available to your child at the school and district levels. These resources promote student academic achievement, and are helpful to parents who may not feel confident supporting their child’s academic learning in the home environment.
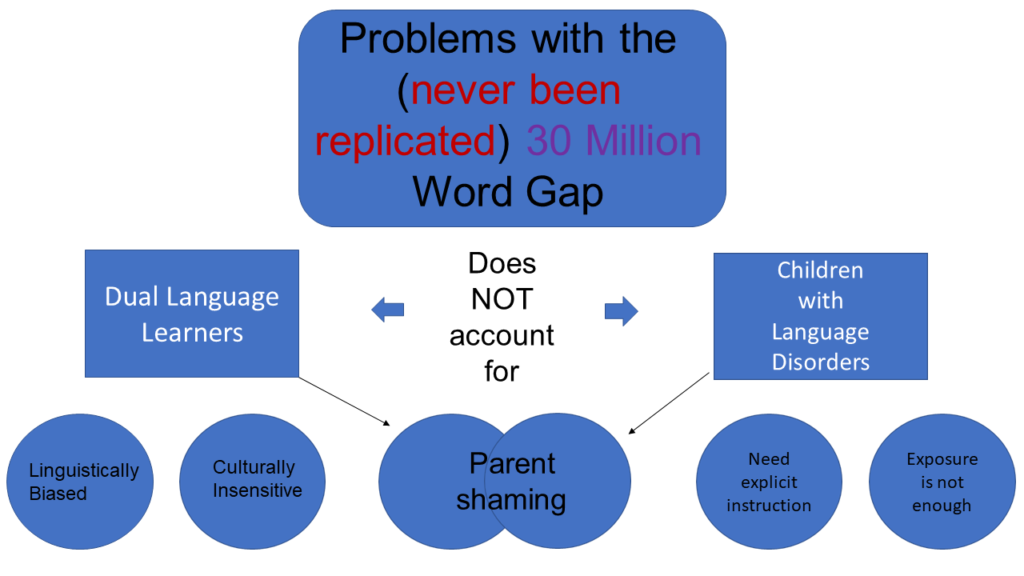
Thank you BOTH SO MUCH! I hope we have provided alternative perspectives that will get professionals thinking instead of blindly re-sharing a catchy research article. In summary, I think we all agree the 30 million word gap is inflated, has never been replicated, is inherently biased, and beyond the catchy headline doesn’t hold a lot of substance or provide any meaningful information. So please everyone, “Mind the Gap” and let’s not fall in feet first.
Kara Mitchell Viesca, PhD is an Associate Professor of Teaching, Learning and Teacher Education at the University of Nebraska Lincoln. Her scholarship focuses on advancing the policy and practice of educator development for teachers, particularly of multilingual learners. She has been awarded $4.6 million in federal funding to support quality teacher learning initiatives for teachers of multilingual students and has published her research in a variety of academic journals. For more information, please visit: https://cehs.unl.edu/tlte/faculty/kara-viesca/
Teresa Rizzi Gillespie, M.S., C.C.C., CBIS, is a Certified, Bilingual Speech-Language Pathologist and a Certified Brain Injury Specialist. She received her Bachelor of Arts degree in Speech Pathology and Spanish from the University of Denver. Teresa received her Master of Science degree from Vanderbilt University, Department of Otolaryngology and Hearing and Speech Sciences. She is currently pursuing Advanced Certification in Bilingual Speech-Language Pathology through the Bilingual Speech-Language Pathology Extension Institute, Teachers College, Columbia University. Teresa has been providing speech-language services to Kindergarten – 12th grade students in the largest public school district in Colorado since 2002. Prior to working in the public schools, she worked at Children’s Hospital Colorado, Rose Medical Center, and in private practice. Teresa has presented English Language Learners with Exceptional Needs (ELLEN) Project trainings through the Colorado Department of Education. She has been a guest lecturer in the Graduate School of Professional Psychology at the University of Denver, Latinx Psychology Specialty, and has served as a Consultant for an online second language acquisition class offered by the same program. Teresa is passionate about meeting the speech-language needs of Dual Language Learners, and consistently advocates for the appropriate assessment and identification of language difference versus language disorder.
Laura Smith, M.A. CCC-SLP is a 2014 graduate of Apraxia Kids Boot Camp, has completed the PROMPT Level 1 training, and the Kaufman Speech to Language Protocol (K-SLP). She has lectured throughout the United States on CAS and related issues. Laura is committed to raising and spreading CAS awareness following her own daughter’s diagnosis of CAS and dyspraxia. She is the apraxia walk coordinator for Denver, and writes for various publications including the ASHA wire blog, The Mighty, and on a website she manages slpmommyofapraxia.com. In 2016, Laura was awarded ASHA’s media award for garnering national media attention around apraxia detailing her encounter with UFC fighter Ronda Rousey, and also received ASHA’s ACE award for her continuing education, specifically in the area of childhood motor speech disorders. Currently, Laura is a practicing SLP specializing in apraxia at her clinic A Mile High Speech Therapy in Aurora, Colorado.