Let’s talk executive functioning. If you follow my facebook page SLPMommyofApraxia (click here), you already know we are making our house an executive functioning friendly zone and you might have read a prior post I wrote a “What is Executive Functioning, and Why Do You Need to Know?”
What does an executive functioning friendly zone mean exactly? I decided to put all of it into a post so you can see and hopefully help others who may have children with similar issues.
Before I begin, I just want to say this:
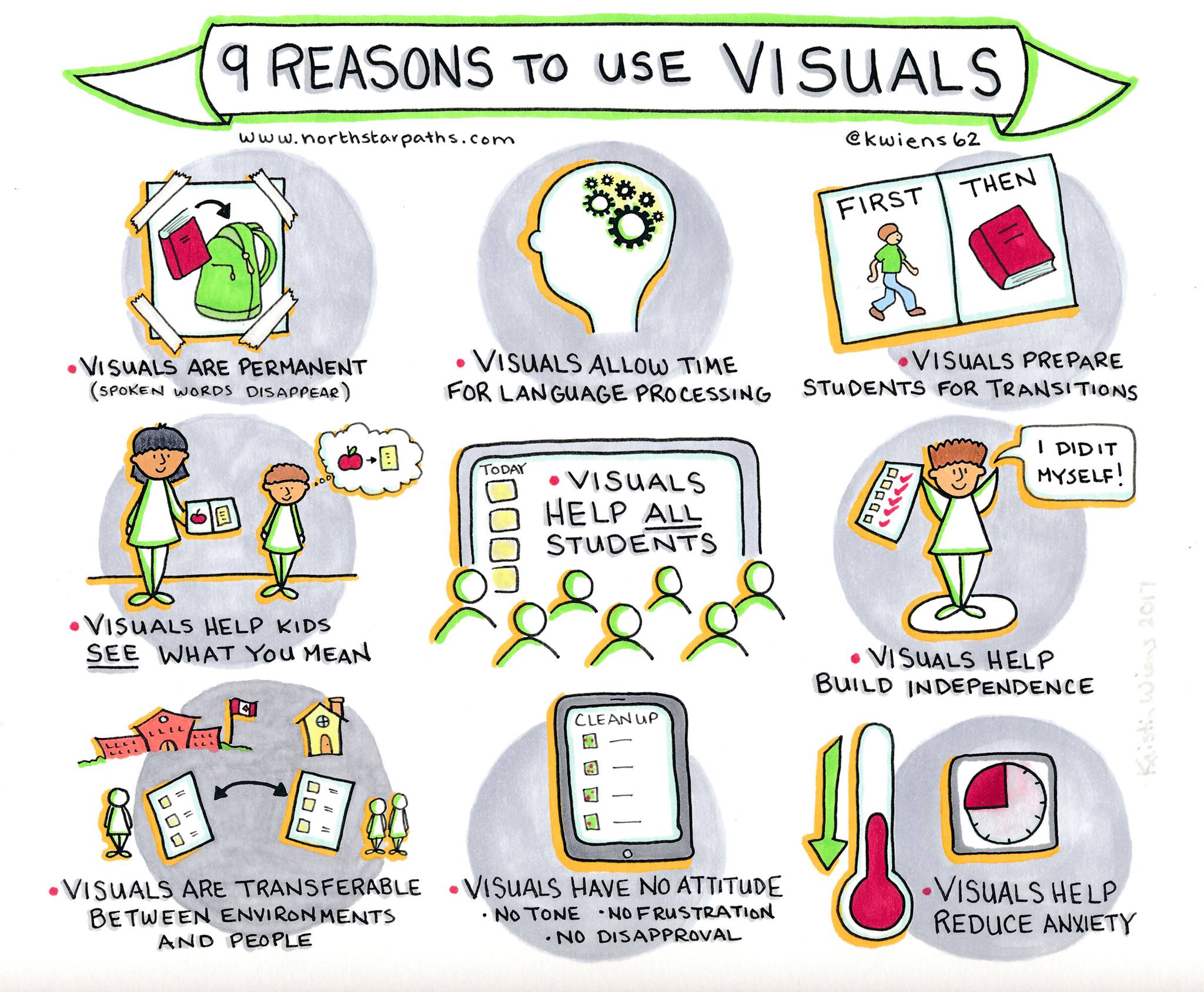
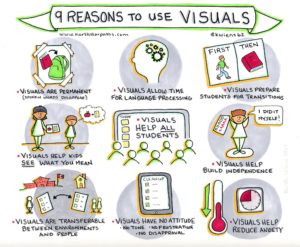
Children with learning differences, many, many, MANY times benefit from the use of visuals. There have a been a handful of cases in my career where visual aids actually confused the student more; but for the most part, visual aids benefit everyone. This visual from northstarpaths really explains why:
Executive functioning (EF) deficits are a common comorbidity with a variety of conditions including: ADHD, OCD, ID and others just to name a few.
Visuals are AMAZINGLY helpful for children with EF dysfunction. The problem is, most teaching involves auditory input. The teacher (or parent) talks, children listen, and learning takes place. For kids like my daughter, who have a language processing impairment, the teacher (or parent) talking is basically the equivalent to the teacher in the Peanuts comic series. All the children hear are “wah wah, wah wah wah wah.”
Visuals bridge the gap. I couldn’t say it better than Benjamin Franklin, who himself had a learning disability when he said,
Aside from just visuals though, kids with EF dysfunction benefit from organization and time management strategies. The following is what we currently have implemented in my home.
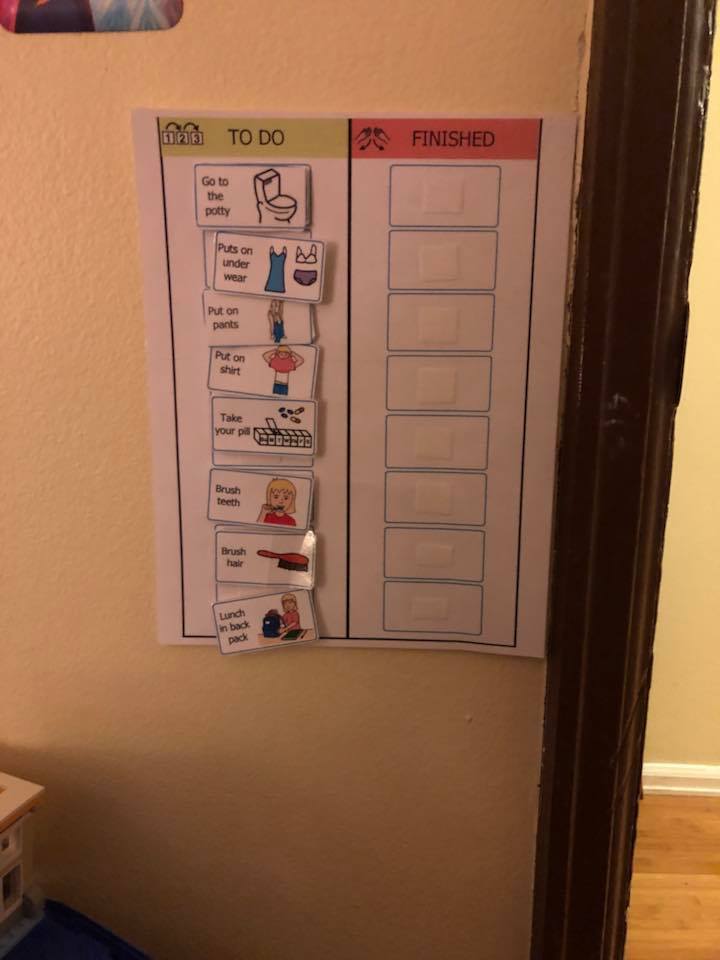
Morning Routine
The most recent example from my personal experience involved the steps to getting ready for school. If I told Ashlynn what to do, she immediately forgot or I had to go through step by step and tell her, which is not promoting independence. With the help of her SPED teacher, we made this visual schedule and she was successfully completing all of her steps without our help in about two weeks.

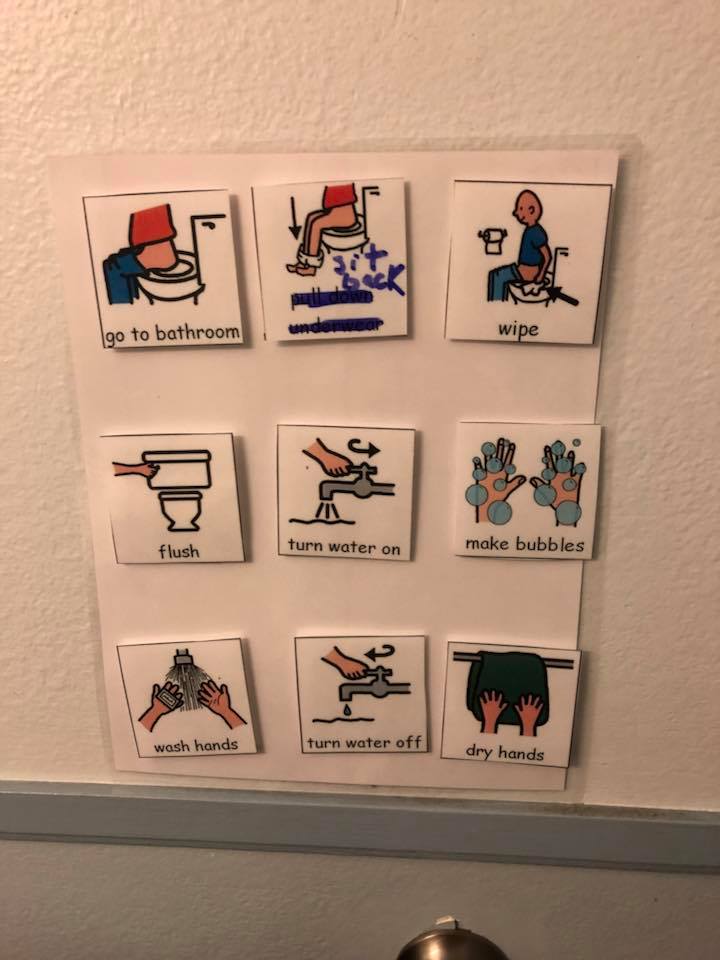
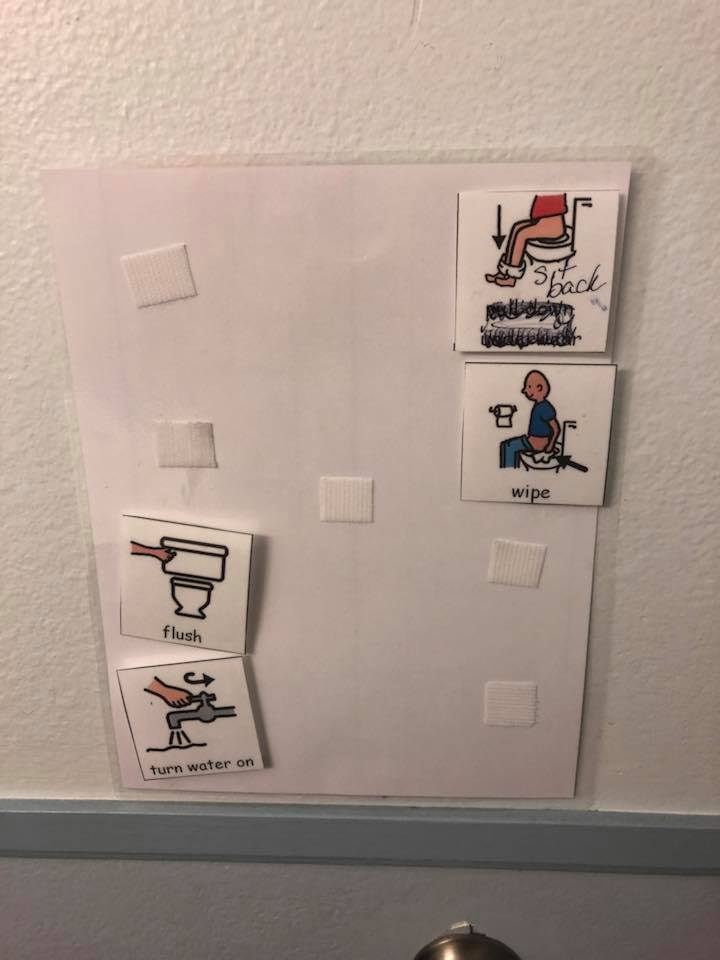
Restroom steps
We decided to make a visual schedule for completing bathroom steps. Let me tell you that we have been working on remembering these for AT LEAST a year. Last year in 2017, I sent her to Adam’s Camp and remember telling the therapists she can say all the steps but still is not consistent. After Adam’s Camp she came home being able to sing them as well, and still, we could not get consistency. So we made a visual schedule a little different than her morning schedule and it looked like this.

This was NOT successful. It probably has too many steps and it doesn’t have the nice left to right motion the morning schedule this, so I modified and made this.

I’d be lying if I said this was a complete success right off the bat, but it has worked better than any other strategy to date and now that the summer has hit, we have made sure she has to go back and complete her steps every single time.
Cleaning her room
The next step was to tackle completing a basic chore like cleaning her room. I can’t even begin to explain the difficulty with this. What I do know, is that many adults with ADHD continue to struggle with disorganization into adulthood. It behooves us now to help our kids develop strategies that are going to serve them well throughout their lives.
The first step is to make sure everything has a place. Classrooms are set up this way for a reason. There is a specific space for each and every item that is used or played with in a classroom. If not, things will inevitibely end up in a pile of clutter. Ashlynn and I went through her room and designated certain drawers and bins for different things. Everything has a spot. There is a bookshelf, a lego bin, a writing utencil drawer, a baby clothes bin, you get the idea.
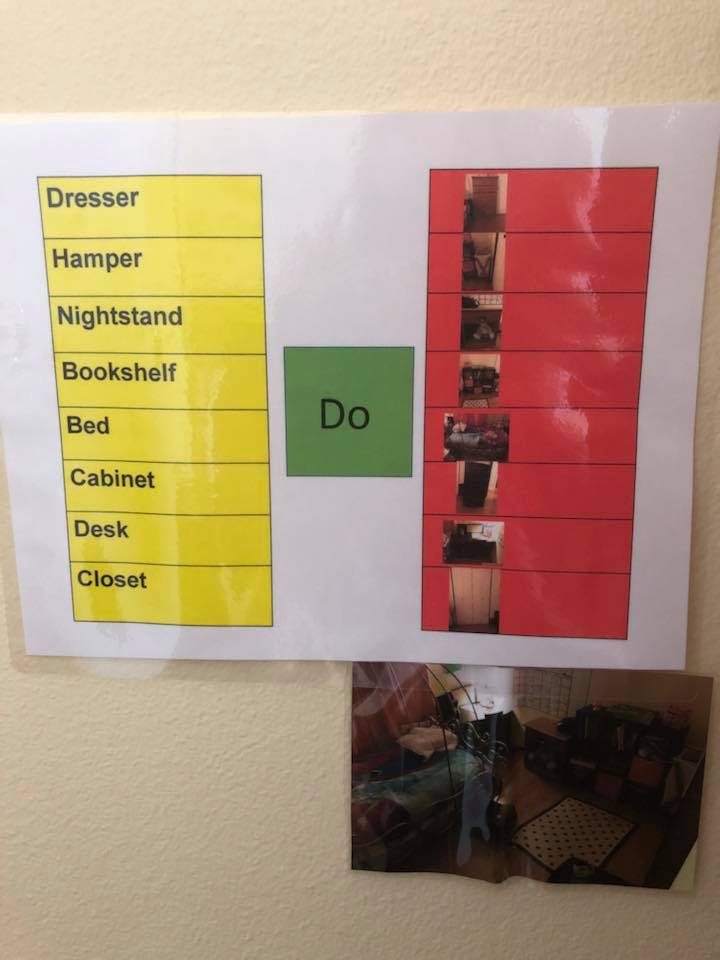
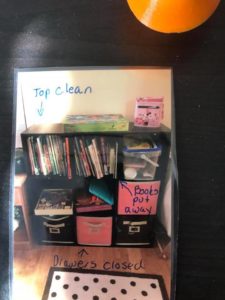
I then created a visual schedule of each piece of furniture that she could check off as she went about her cleaning routine.

I know it’s hard to read, but basically each furniture item is listed on the left, with a picture representation on the right of what it looks like done. The picture on the bottom is a grand finale picture of what the entire room should look like clean after completing all of the steps for one last check.
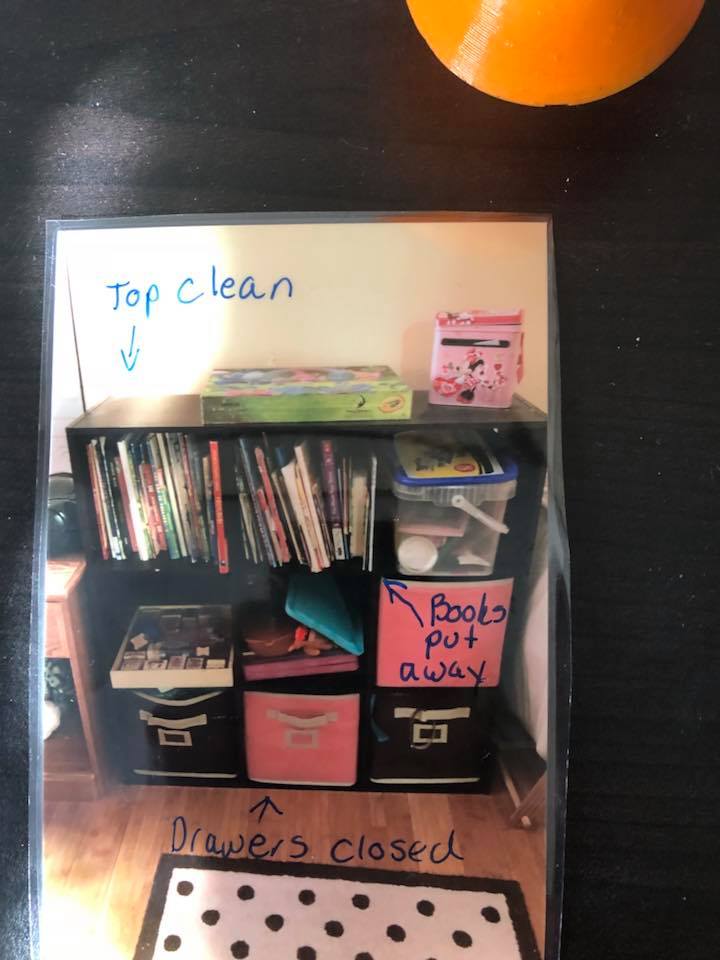
Next up was to have bigger picture velcroed to all of the furniture items so she could see as she was cleaning them what they are supposed to look like. I know it seems redundant, but seriously if you have a child who struggles this, then you will relate when I say that a dresser with closed drawers looks fine with clothes hanging out of it to her. Same with a picked up hamper. I even have a picture showing what the closet should like closed and no that doesn’t mean it is closed until it hits the piles of crap. It means actually closed and looking neat.


I have to add that these helped, but still had to be taught. In fact, it’s still a work in progress. Some nights, I am so frustrated and just want to pull my hair my out. I’m only human after all. I do though, in those times, try and decompress and remind myself this is not a *fix* but a lesson. Ashlynn doesn’t learn like other kids and that’s okay. I have to realize though that all of this will pay off in the long run, and when we start early kids have the best outcomes.
Homework
Oh man don’t we hear horror stories about homework from parents of kids with varying learning differences. Teachers make homework sound so easy. Ten minutes for every grade you are in, so a first grader shouldn’t be more than 10 minutes a night.
Say….what??? That assignment just took my kid an hour….and then when we went to second grade, that so called 20 minute assignment just took upwards off and on of two HOURS? Minutes? What?
Know that homework can always be modified, but there are strategies that can be put in place to help with this too. Number one is to just start with a place that is going to make them successful for learning. If you are like me, my first baby is the one with learning differences so instead of preparing for the ultimate learning environment, we were more focused on transitioning my son from a crib to a toddler bed and spent our money on that. Needless to say, our kitchen table became her homework place. Yes, the place that she eats and the chair in which she sits that her feet don’t touch on the ground yet is what we thought would be the perfect location for her to sit down and do that quick assignment in 10 minutes. I should mention too it’s a thoroughfare in my house, so my kid with ADHD was also constantly distracted by the events taking place all around her. Can we talk about set up to fail???
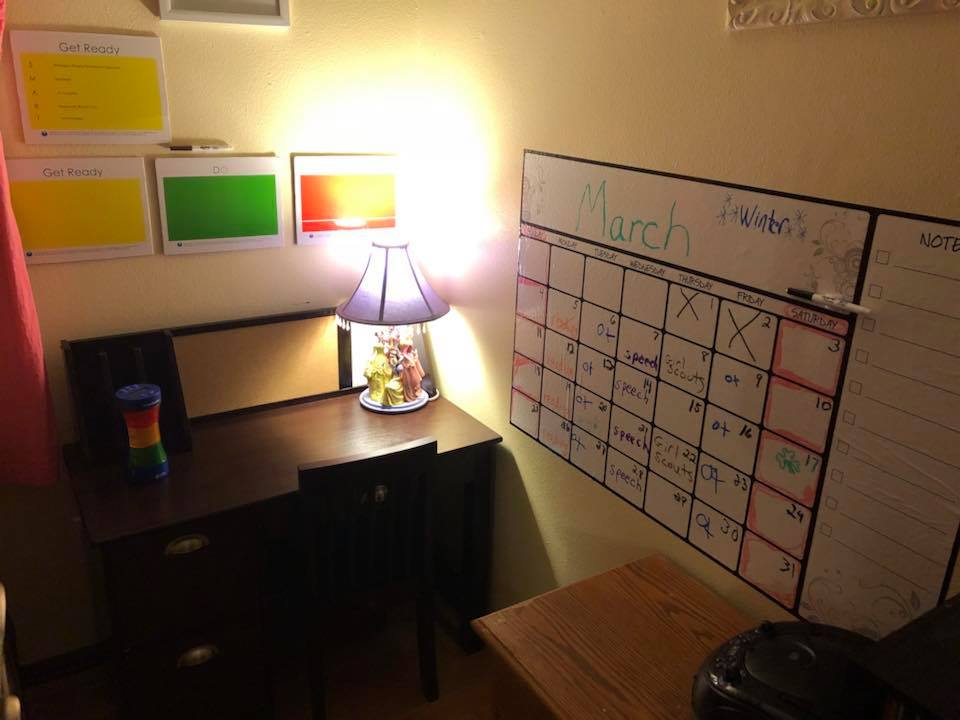
I redid her room and created a homework corner. I bought her a new desk in which she sat at a 90 degree angle, perpendicular to the floor, and decked it out with strategies from executive functioning queen Sarah Ward from the website Cognitive Connections.

New desk with feet on the floor
As you can see, I have her own desk, in a corner of her own room, that is quiet and in which her feet touch the floor!
Get ready, do, done boards
The colored board above the desk are suggestions from the cognitive connections website. In the yellow, we write everything we need to get ready. It might be as simple as a pencil and it might be more complicated if doing a project. (To modify for non-readers, you can tape or velcro pictures that you need.).
The green stands for “doing.” These are the steps you need to do to reach the finished project. The finished project then is the red board and reflects what the assignment looks like when it is finished. For lower level, you can put a picture of what a completed assignment looks like, or for readers you can simply write it. Sarah Ward also recommends to “start with the end in mind,” meaning kid with EF deficits benefit from knowing what the end is supposed to look like and then working backwards. For a more elaborate description, go see Sarah Ward talk. She’s amazing.
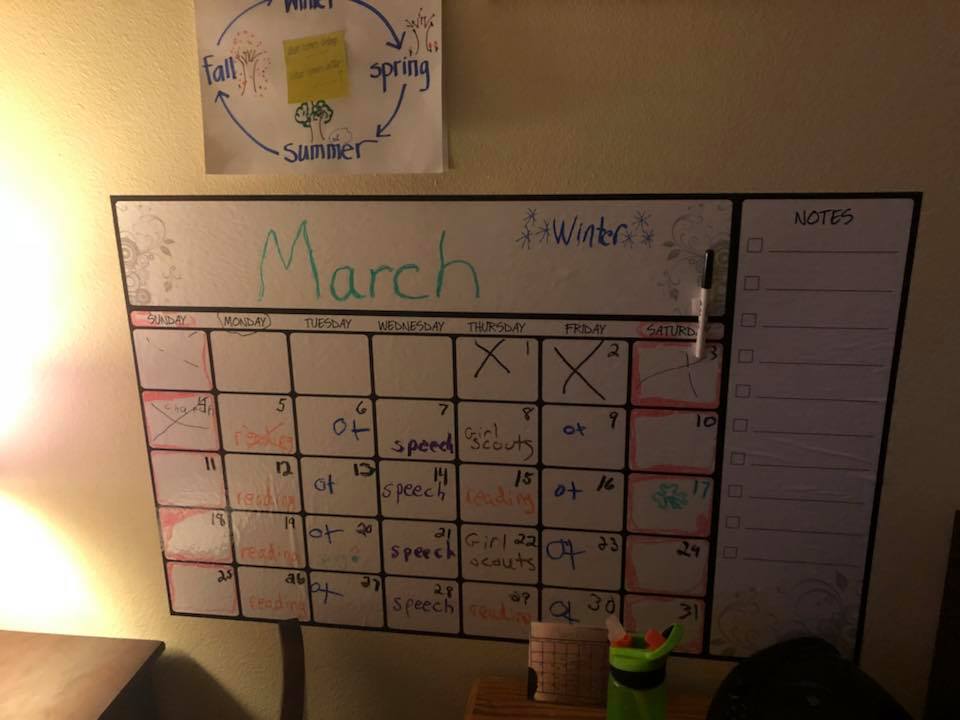
Calendar
We have tried a few different things to help Ashlynn learn time, and I’m not just talking time management. Ashlynn has had a lot of difficulty learning the seasons, days of the weeks, the months, and understanding the difference between yesterday, today, tomorrow, last week, next week etc.

I decided to buy this peeling dry erase calendar at target. It’s huge and sits right by her desk. Every month, she helps me write the month and the days. We then go through and write her therapy/activity schedule and color code them. Each activity is written in a different color. The weekends are shaded on red since she has a difficult time understanding that Saturday and Sunday are one unit (the weekend) when they are split up on a normal calendar. We then marked an X for each day that had passed and talked about yesterday and tomorrow. This calendar has been AMAZING. I might be so bold as to say it almost helped her understand days of the week right away.
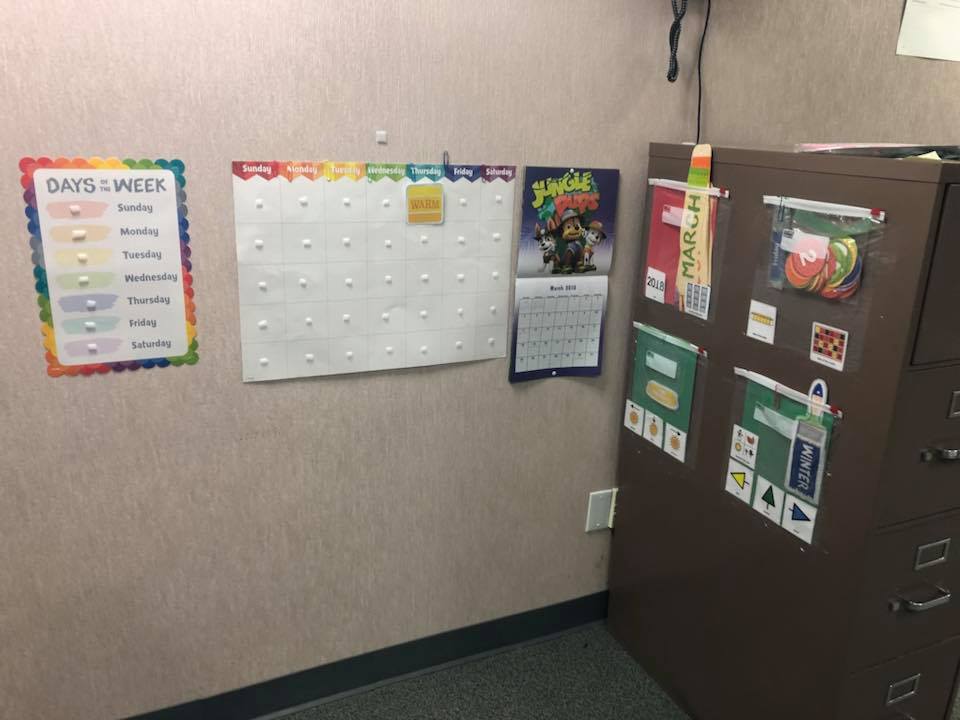
Her school though also hit this hard visually and created the following corner in the SPED room just for her.
 ‘
‘
This picture is also hard to see, but basically you see the basic calendar color coded by day in the middle. To the left, each day of the week is color coded. On the file cabinet on the right, the months are placed and she has to pick out the right month each day for added repetition. The days are in the second bag, and there are tiles for the season and then arrows to talk about the concepts yesterday and tomorrow. A normal calendar was provided as a reference to keep track of how her modified calendar related to a typical calendar.
Timer
Last to come is the timer I used for all of these tasks! Time management is another HUGE skill that is difficult for those with EF deficits.
The timer is from the autism community store here in Denver, but I’m sure you can find them on Amazon or other places. This timer is amazing!! The colors stand for different things similar to a stoplight. Green means go, yellow means caution you are nearing the end, and red means you need to be done or stop NOW. What is best, is that each color is completely customizable by time. For her morning routine, we usually set it for 3-3-3. For homework, it might be 2-20-2. Did I mention it also comes with sound? So that means every color it changes to also has a sound to go with it, aka, an auditory cue.

The impact
I have to admit, there were times that as even I were making all of these materials and buying all these things that I wondered will this really make a difference? Was all this work really worth it?? My answer came from Ashlynn. As I was making these visuals, she probably thanked me more than 10 times. She knows how she learns. She was just waiting on me to help her.
Laura Smith is a mom to two children, one of which who has multiple learning differences. She is also an SLP (speech/language pathologist) specializing in CAS (Childhood Apraxia of Speech), a passion that was fueled by her daughter’s dx in 2012. To learn more, visit slpmommyofapraxia.