Ashlynn is in 2nd grade and is in Girl Scouts. She has been in Girls Scouts since Kindergarten. She loves it; but honestly, Ashlynn loves most activities and new adventures. Yes she has apraxia, dyspraxia, SPD, ADHD, learning disabilities and a language processing disorder; but despite all of those disabilities she is a true extrovert that one.
Ashlynn’s Girl Scout troop leader is seriously amazing. If there were an award, I would nominate her to be the best girl scout troop leader in the state, because she is. A girl scout troop leader is a volunteer who donates their time. This woman though I think must be a real life saint who deserves a salary. When Ashlynn first started Girl Scouts I wrote a post about how she became misty eyed and told me that she knew what Ashlynn was going through.
When I first met her, I noticed something a little off with her speech. Later I found out she has a hearing disability, and has had one since birth. From the beginning she was very concerned about Ashlynn’s needs. I was also surprised to learn that she had never had anyone with a disability before. She told me she just wanted to make sure this experience was the best possible experience for her, and that she was willing to make accommodations or help her however she could. We ended up having to make a few accommodations, especially with requirements. For example, in Kindergarten the girls needed to have memorized their name AND address to earn a special pin. It took everything we could do for Ashlynn to learn the address, but we could just not get the phone number at that time. Ms. E made an accommodation like a trained special education teacher would; and said as long as she can memorize one of the two, she would earn her pin.
The other night the girls had homework. It was a picture where you had to find items hidden in the picture. She sent home the actual picture; and then she found, on her own, a simpler picture and told me that Ashlynn just had to finish one. In special education we call this modifying the curriculum. This woman has never read Ashlynn’s IEP. She does not in fact know her modifications or accommodations. She intuitively does them. I can’t help but think it’s because she understands. She has walked Ashlynn’s shoes. She totally, totally gets it.
This past weekend there was an event at the Denver Zoo called “Bunk with the Beasts.” The girls would get to spend a night away from home and “camp” at the zoo. Right after I received the group email about the event, her troop leader followed up with a personal email requesting that she know of any special accommodations or help that Ashlynn would need so she could do them. She didn’t want Ashlynn to miss out. I sent back a big list. Ashlynn has dyspraxia. Activities of daily living, like all the steps to get ready for bed are NOT easy. Her troop leader wrote back it wouldn’t be a problem. A few days later a chaperone pulled out so I was asked to come. I was thrilled! I said yes immediately. This way her troop leader could focus on the other 18 girls, and I could be there and help Ashlynn.

When we arrived, there were 4 adults to 19 girls. Her troop leader split them into groups of two. She told me that usually a chaperone or leader is not placed with their girl, but in this case she made an exception. So her and I were in charge of one group of girls in which Ashlynn was a part of, and the other two co scout leaders were in charge of the other group of girls for the zoo tour and excursions. Some would find this preferential treatment; but it is in fact, an accommodation. I found a renewed sense of awe in this woman. She went onto explain that many of the girls have developed “best friends” and she purposefully separated them for this event because a troop cannot be a troop unless they all learn how to work together. I shrugged it off. She looked at me more earnestly and said, “No, when I mean best friends I mean like this,” and she proceeded to hug my arm and not let go. I still shrugged it off not realizing yet her point.
As she gathered the girls and called out what group they were in, one of the girls was visibly shaken. Her mom is a girl scout troop co-leader and I was standing next to her at the time. She told me that this was a big reason her daughter wants to quit Girl Scouts next year, because Ms. E insists that the girls be separated from their best friends. As she talked I looked on. Most girls had a best friend in which they were sitting next too. If not, they were still obviously part of the group. Two girls sat in the back of the group slightly removed, but Ashlynn was basically completely removed in the back by herself. Don’t get me wrong, she wasn’t acting upset or lonely. Ashlynn loves girl scouts. It just struck me in that moment that most girls had an “arm clinging” best friend, and my daughter had no one. This mother I was standing next to felt so bad her daughter would feel alone and away from her best friend for a couple of excursions, and my daughter felt that way basically all the time. I don’t fault this mom. Maybe if I didn’t have a kid with a disability, I would feel the same way too. Maybe I wouldn’t understand or even notice that another child in the group, the child with disabilities never had any of those best friend moments. Maybe I would be sad that my child would be sad for a couple hours and never realize this girl in the same troop sitting in the back by herself doesn’t EVER have an “arm hugging” best friend. Maybe…..
Ms. E did though. Ms. E noticed. That’s why she split them up. Society needs to stop casting those who are different to the outside, but including them and accepting them too! We are all better when we work together. Ashlynn and I had the best time. Ms. E paired each child with a “buddy” and Ashlynn was thrilled to have a peer’s hand to hold as she walked around the zoo. Ashlynn’s joy is so contagious and she is an adult magnet. I could see though in this setting, just how unlike her peers she looks. She’s not shy. She doesn’t get embarrassed or worried about making mistakes. She bonks into stuff and people and laughs at herself. She loses attention easily and starts to wander which would annoy her buddy. She would randomly start talking or singing when you weren’t supposed to and her buddy would have to shush her. It didn’t matter though. It made Ashlynn’s entire night to be part of her peer group.

I came home and cried to my husband I get why girls think she’s different. She’s not stuck up. She’s not concerned about what other people think. It’s amazing how society gets it’s grasp into children as young as second grade. I noticed so many girls tugging at their shirts, checking their appearance, and censoring what they say because they want to fit in. I couldn’t help but look at Ashlynn and think of the Dr. Seuss quote, “Why fit in when you were born to stand out?”
What’s ironic is these kids who “stand out” end up changing the world. I am almost obsessed with successful people. Notice I didn’t say “famous” people, though many might be famous. No SUCCESSFUL people. People actually changing the world and making it a better place. The innovators and visionaries. Most of them were kids who were a little different. Some may have had a “disability” like ADHD, dyslexia, or whatever. Bill Gates said once, “Be nice to the nerds. You might end up working for them.”
Last month in the news the boy scouts were under fire for revoking the eagle scout badge for a teen with Down Syndrome. The parents filed a lawsuit claiming that their son was being discriminated against because without accommodations, there would be no way he could earn the necessary requirements to get the Eagle Scout Award.
The argument against him earning the award was that though he tried his hardest, he did not meet the requirements set forth. If you don’t have a person with a disability in your family, I could see how this could make sense to you. There are requirements that have been established, and if a person can’t meet them for whatever reason, they don’t. There are able bodied children who don’t meet the requirements either and that’s just the way it is, right?
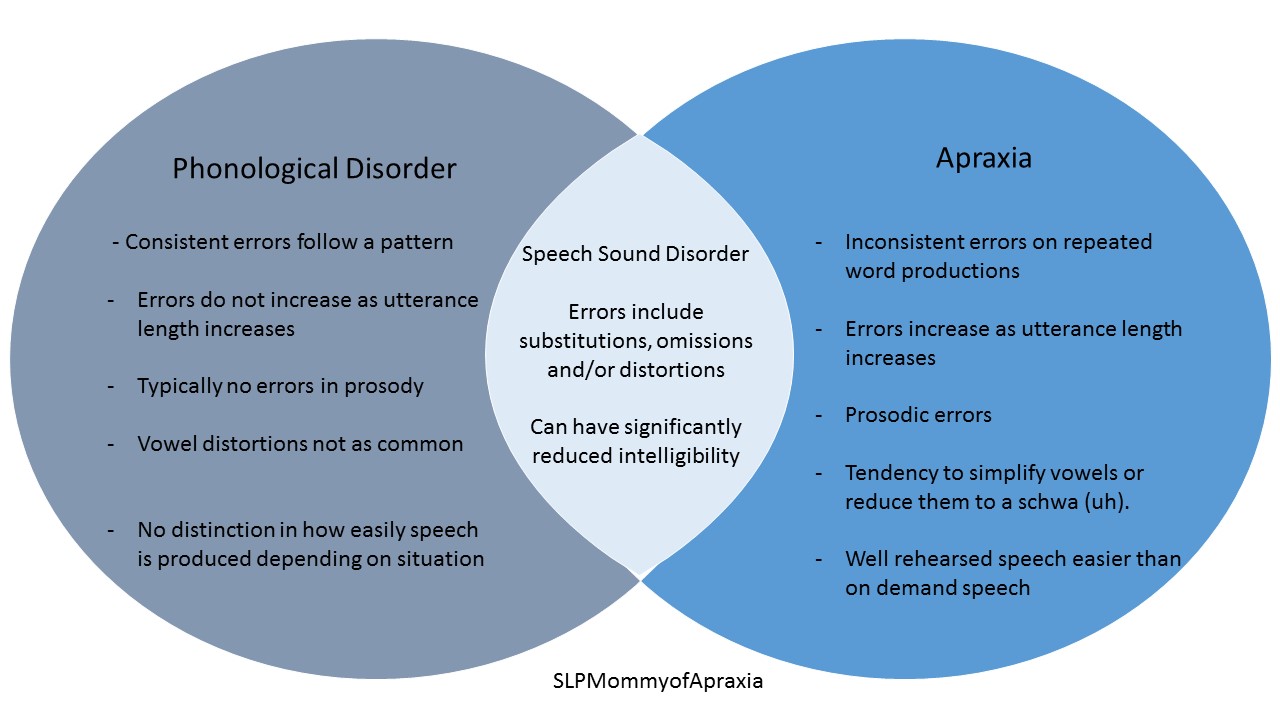
Let me point out this graphic.
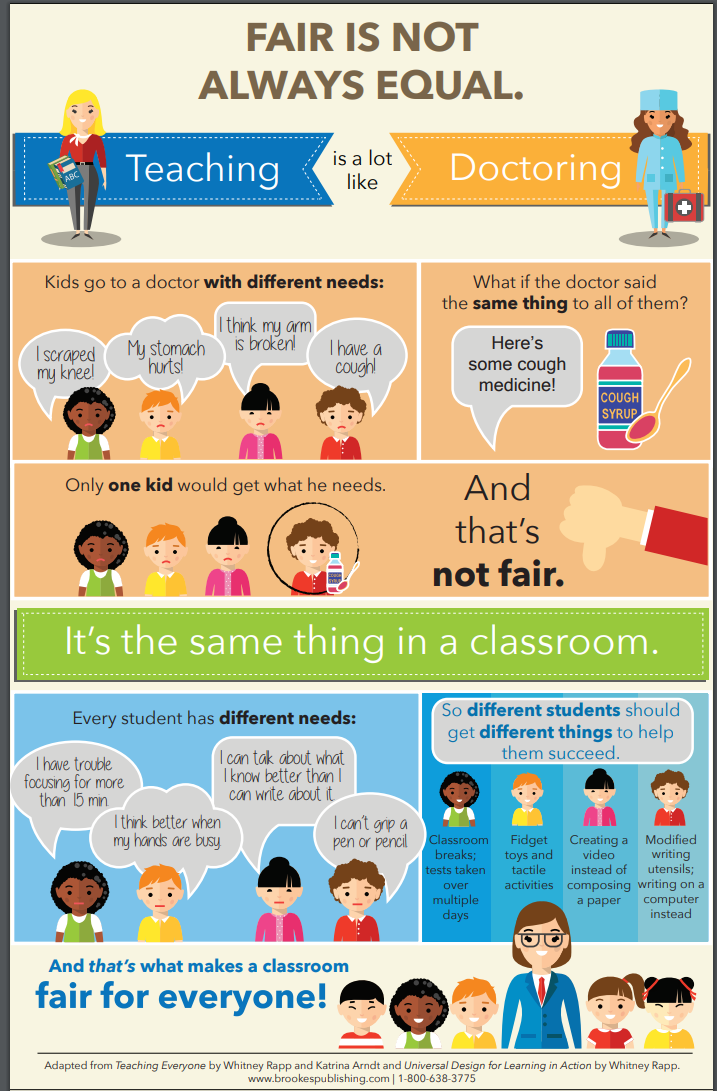
This graphic compares teaching to going to a doctor. Kids go to the doctor for different symptoms, and the doctor treats the symptoms. It would be ridiculous though if you went in with a broken arm and the doctor prescribed antibiotics. Under our current educational model that is not inherently inclusive; this is exactly what is happening. The current educational model is based on a child without any learning, attention, or behavioral disabilities. The lessons are made and the classrooms are set up for kids who can sit in a chair, listen and interpret information, and then attend to their work. It is not equipped for the child who needs sensory breaks, or the child who needs to use asisstive technology to help them write because they can’t, or the child who needs assistive technology to have something read to them because they can’t read. It is not set up for the child who cannot learn through the auditory channel but learns best through visual and tactile channels. Here is the most important piece though about all of this. Children who are not “typical” CAN show their learning and skills in other ways if they are just given accommodations!!
That’s not fair, you might say. I would counter that it’s not fair we have a bunch of children with broken arms (learning disabilities) being forced to take antibiotics (traditional education), and then are penalized for failing. They are SET UP to fail. A system that mandates all children must learn the same and prove they have learned the same is a broken, discriminatory system. As Albert Einstein once said, “If you judge a fish by it’s ability to climb a tree, it will spend it’s whole life thinking it is stupid.”
Ms. E understands this and I am so, so thankful to her. The challenge today for apraxia awareness month was to recognize a teacher making a difference. There are so many amazing people I could choose, but today I Thank you Ms. E, for recognizing my daughter is a fish and deserves a chance to swim.