I’m so honored and excited to have Dr. Kathy Jakielski, Ph.D., CCC-SLP with me today! I met Dr. Jakielski at the CASANA Intensive Training Institute, as she was one of the instructors.
The honor is all mine, Laura. Thank you for your interest in my work!
Kathy, I remember vividly this moment at the end of the training, where we all sat around a big conference table, and you gave an impassioned plea. You expressed worry over the future of apraxia, and families having access to quality, research-based intervention. You worried who was going to carry the torch; and as a mother to a child with apraxia, I felt so much gratitude that there were people in this world like you who cared that deeply about a rare speech disorder many have never even heard of.
When I saw that you had put out your own toolkit, I wasn’t surprised at all to see that you teamed up with CASANA so that proceeds would benefit the non-profit dedicated exclusively to Childhood Apraxia of Speech and their families. Will you tell us what made you decide to dedicate all proceeds to CASANA programs and research?
Two reasons. The first is because I deeply appreciate CASANA. Before CASANA was founded, parents of children with CAS had to scour articles and conferences to identify researchers experienced with this relatively rare disorder. Parents then would contact us directly via phone and email with their questions. A single correspondence with a parent seeking basic information could take up to an hour, and additional correspondence often was required to answer follow-up questions. There were not enough hours in a week to correspond with all the families seeking information, and I was disheartened that I couldn’t answer more calls. CASANA changed that. From a practical standpoint, they saved me time, while providing families with the information that they needed to make decisions for their children with CAS. Partnering with CASANA on this project was a way to give back to an organization that exists solely to provide and advance education about CAS.
The second reason, and perhaps the most important one, is because I trust CASANA. I tell parents all the time that they can go to the apraxia-kids website and trust anything they discover and read there. I also knew that they would produce a high-quality product and protect the integrity of my work.
Please tell my readers a little more about your background and how is it you came to specialize in CAS.
My initial contact with CAS was when I was working as a clinical speech-language pathologist in private practice. I treated my first child with CAS in 1984, right after I finished my master’s degree program. There was so little information on CAS at that time, but some of the early researchers, Drs. Barbara Davis, Tom Marquardt, and Harvey Sussman, were at my master’s degree institution, so I was able to participate in some of those early studies. But it was by working clinically with several children with this frustrating motor speech disorder that I really came to know and love its challenges. Working clinically for nine years left me with more questions than answers, so I returned to graduate school to pursue my doctoral degree. The work I began in my doctoral program, researching typical and disordered acquisition of speech, as well as differential diagnosis of CAS, are areas of inquiry I continue to study even today.
You have recently developed and published a new toolkit used to treat CAS. Is this a treatment plan also (and if not, what approach do you use)? What is it and will you please briefly describe it?
 Building Speech and Quantifying Complexity (BSQC) is a systematic approach for developing therapy goals and selecting words and phrases to target in treatment on a child-by-child basis. It is not a treatment technique, but rather, a phonetics-based approach for deciding what to work on in therapy, but not how to work on it.
Building Speech and Quantifying Complexity (BSQC) is a systematic approach for developing therapy goals and selecting words and phrases to target in treatment on a child-by-child basis. It is not a treatment technique, but rather, a phonetics-based approach for deciding what to work on in therapy, but not how to work on it.
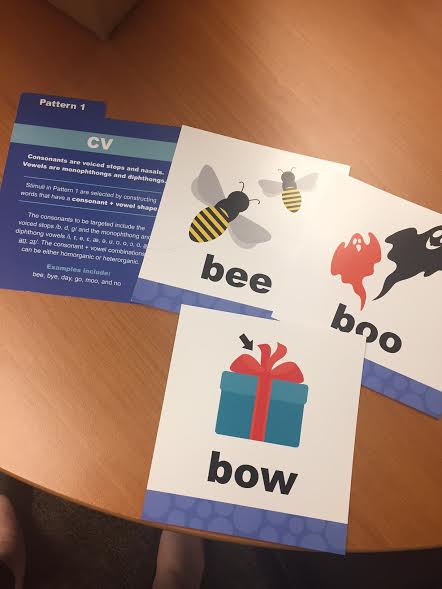
Several therapy techniques (e.g., PROMPT, DTTC, etc.) have been found to be efficacious for how speech-language pathologists can conduct their therapy; however, selecting an evidence-based technique is only one part of clinical practice. Speech-language pathologists also need to be able to select the stimuli that they will target while employing a specific technique. This is the gap that BSQC fills. BSQC is an approach that speech-language pathologists can use to select the goals and stimuli they will target in therapy for children in the early stages of speech intervention. The approach consists of eight speech patterns, or speech frames, and the stimuli that can be used to teach and practice each frame. I have found that many speech-language pathologists do not know how to hierarchically structure the phonetic complexity of speech goals and stimuli for children with severe speech sound disorders, such as CAS. While a speech-language pathologist might be very proficient using various articulatory techniques, if the words targeted are not within the child’s set of motor speech capability, then the child’s progress will be limited and therapy can stall.
 BSQC serves three primary functions. It is designed to help speech-language pathologists: 1) assess a child’s motor speech complexity over time; 2) develop speech goals that become developmentally and phonetically more complex over time; and 3) develop functional stimuli (words and phrases) to achieve each goal.
BSQC serves three primary functions. It is designed to help speech-language pathologists: 1) assess a child’s motor speech complexity over time; 2) develop speech goals that become developmentally and phonetically more complex over time; and 3) develop functional stimuli (words and phrases) to achieve each goal.
Current research indicates principles of motor learning should drive therapy approaches for CAS. Are principles of motor learning incorporated into BSQC?
Leave it to a CASANA boot camp graduate to ask that great question! Yes, speech-language pathologists want to consider the principles of motor learning as they conduct intervention using BSQC or any other approach. As previously described, the BSQC toolkit is not a therapy technique, but rather, is used to develop the goals and accompanying stimuli for intervention. Speech-language pathologists need to apply principles of motor learning to the technique they employ. It’s easy to do using BSQC, as there are probably close to 1,000 possible stimuli across the eight speech patterns that speech-language pathologists can use to teach each frame.
How does your toolkit incorporate current evidence based practice?
BSQC has grown directly out of the rich research literature on the early acquisition of consonants, vowels, and word shapes produced by typically-developing children in babbling, jargon, and early words. The eight speech frames and accompanying stimuli are based on this body of research, along with some of the cognitive motor learning literature. BSQC also provides speech-language pathologists with a sensitive measure for tracking articulatory progress in speech. This measure, the Index of Phonetic Complexity, has been used in some research for the past 20 years; however, this is the first time I am promoting it for clinical use.
Can any SLP start using this toolkit or is there some training or manual that is recommended first? Are you offering any workshops or trainings? Finally, is this toolkit appropriate for parents to buy also and use at home?
The toolkit includes a manual that explains the Building Speech materials, which include the goal and stimuli development. The manual also explains the Quantifying Complexity measure, the Index of Phonetic Complexity. In addition to the easy-to-follow manual, there also are close to 800 bright, colorful, child-friendly picture cards depicting many of the words a speech-language pathologist could target using the BSQC approach. The BSQC approach is not appropriate for parents to buy and use at home because of the phonetics background required to understand it, as well as needing to possess knowledge of speech intervention techniques.
CAS master clinician Lisa Mitchell, M.S., CCC-SLP and I gave a webinar for CASANA on the BSQC approach, which is available for viewing at the apraxia-kids website. I also teach the approach in an online course that’s available through MedBridge, a continuing education company at www.medbridgeeducation.com. In both courses, I explain each step of the approaches, and then you see Lisa putting the approach into action with children on her caseload, which is the real highlight of these presentations.
Lisa and I also will be teaching the BSQC approach at CASANA’s 2017 Annual Conference on CAS to be held in San Diego, California from July 6-8. Lisa and I will be presenting a pre-conference workshop on Thursday, July 6th. I highly recommend this annual conference to speech-language pathologists and families.
Therapy for CAS in very individualized due to each child’s unique phonetic and syllabic repertoire, but also should take into account personalized and functional words relevant to each individual child. Can you explain how your toolkit accounts for this?
I designed the BSQC approach to be individualizable and flexible. There are a myriad of stimuli that can be developed to target each of the eight speech frames, some included in the kit as picture cards, but the key is to determine which words will give a particular child increased communicative power.
The steps for utilizing the BSQC approach follow.
1) Phonetically transcribe a representative speech sample from a child and analyze it to determine the child’s phonetic repertoire.
2) Examine the phonetic repertoire to determine which of the BSQC eight speech frames you need to target, and in which order.
3) Develop a list of functional words and phrases for that particular child to teach each of the speech frames you decided to target.
4) Determine the therapy technique you will use in therapy, and incorporate principles of motor learning as you design your sessions.
5) Use the Index of Phonetic Complexity to quantify incremental progress in speech skills over time. The sensitivity of this measure can help document change that can be used to show progress.
What sets this toolkit apart from other cards out there marketed toward apraxia?
This therapy kit provides a unique way of hierarchically ordering speech stimuli based on speech acquisition research. The speech measure, the Index of Phonetic Complexity, purports to measure the phonetic complexity of a child’s speech, which is a very unique feature.
Thank you for agreeing to offer one today for a giveaway! Where can my readers go to buy this product, and for my International readers, can this product be shipped to other countries?
Go to www.apraxia-kids.org to place an order. International readers can email CASANA directly for information regarding shipping BSQC to other countries; however, please note that BSQC was developed for American English, and while easily adapted to different dialects of English, it is not intended to be used for languages other than English.
Kathy, thank you so much for being here! I also can’t thank you enough for all you have done to advance the field of speech/language pathology, especially in the area of Childhood Apraxia of Speech. I’m honored to call you one of my mentors.
Thank you, Laura, it’s been my pleasure. Thank you for wanting to find out more about BSQC. And thank you, also, for the wonderful clinical, educational, and family work that you offer!
 Kathy J. Jakielski, Ph.D., CCC-SLP is the Florence C. and Dr. John E. Wertz Professor in Liberal Arts and Sciences at Augustana College in Rock Island, Illinois where she serves as Chair of the Department of Communication Sciences and Disorders. She has over 35 years of clinical experience working with children, adolescents, and young adults with severe speech impairment, including CAS. She currently conducts research on genetic bases, differential diagnosis, and intervention efficacy on children with CAS. Teaching the next generation of SLPs and thinking about CAS is what gets her out of bed in the morning.
Kathy J. Jakielski, Ph.D., CCC-SLP is the Florence C. and Dr. John E. Wertz Professor in Liberal Arts and Sciences at Augustana College in Rock Island, Illinois where she serves as Chair of the Department of Communication Sciences and Disorders. She has over 35 years of clinical experience working with children, adolescents, and young adults with severe speech impairment, including CAS. She currently conducts research on genetic bases, differential diagnosis, and intervention efficacy on children with CAS. Teaching the next generation of SLPs and thinking about CAS is what gets her out of bed in the morning.
Enter the giveaway below! This is over $175.00 value! Please note this toolkit is specially designed for SLP’s. If you are a parent and enter the contest, please give to your child’s SLP! Thank you!
*Note – this giveaway is now closed*
a Rafflecopter giveaway