Apraxia? Phonological Disorder? Language Disorder? What’s the difference?
So many times I see parents post a video of their child speaking, or attempting to speak, and they ask, “Is this apraxia?”
The follow up question is usually something like, “If it’s not apraxia, then what ELSE could it be?
The answer is that childhood speech and language delays can be caused by a variety of factors. It’s important to keep in mind too, the difference between “speech” and “language” disorders when we are discussing speech and language delays.
On the surface, speech and language seem like different sides of the same coin. This is particularly true when people or even professionals may seem to use the terms interchangeably. If a child isn’t speaking, they must have a “speech” problem right?
Not necessarily.
A child with a “speech disorder” has a problem in the way or how they say sounds. Most of you who read this blog know my daughter has apraxia, and apraxia, in its truest sense, is a “speech” disorder. It’s not a language disorder (although my dear daughter and many other kids have both). Other common factors that can cause speech disorders, or the way kids say their sounds are:
1.) A hearing loss, or even a history of chronic ear infections – If a child has a hearing loss, or is suffering from a hearing loss due to chronic ear infections; their typical speech development *may* be negatively impacted. Without going into a technical explanation, it makes sense that a child with ear infections who is hearing like they’re “under water” during the time they are supposed to be learning how to talk, may have speech and/or language development that is delayed.
2.) Stuttering – a disruption to the flow of speech, is also considered a “speech” disorder because it is characterized by disruptions in the production of “speech sounds.”
3.) Phonological Disorder – Phonological disorder is one of the most common speech disorders that SLP’s treat, so I was shocked to go to the ASHA website and find this definition:
Speech sound disorders that impact the way speech sounds (phonemes) function within a language are traditionally referred to as phonological disorders; they result from impairments in the phonological representation of speech sounds and speech segments—the system that generates and uses phonemes and phoneme rules and patterns within the context of spoken language.
It is NOT that complicated. To put it simply, phonological disorder is a speech sound disorder in which the child typically makes consistent patterns of errors. For example, one common phonological process is called fronting. In this process, the child will consistently produce the /k/ sound as a /t/ sound, and the /g/ sound as a /d/ sound. It is a predictable, patterned error. This child, regardless of the word will usually always make these substitutions. However, a child with a phonological disorder can have several phonological processes they are employing and be quite severe and have significantly reduced intelligibility. A child with phonological disorder may have numerous substitutions, omissions, or distortions.
4.) A motor speech disorder such as apraxia or dysathria – Apraxia of speech refers to a child’s difficulty with the planning and programming of speech production that results in inconsistent errors, deficits with prosody, and significantly reduced intelligibility. Unlike kids with phonological disorder, children with apraxia do not always have predictable and consistent error patterns. This could be on repeated productions of the same word, or the ability to produce one sound in different words.
For example, a child with apraxia may be able to say an /m/ in the word “momma,” but be unable to say or inconsistently say an /m/ in the word “more.” Another child with apraxia may say “baby” for baby once, but when asked to say it multiple times may produce it different ways such as saying: baby, bay-ee, daby, or day-ee. A child with apraxia may have numerous substitutions, omissions, or distortions.
In addition, children with apraxia have some sort of prosodic disturbance to their speech. This can manifest in ways such as: stressing each syllable in a word resulting in more “staccato” sounding speech, or errors with pitch, intonation, rate or volume.
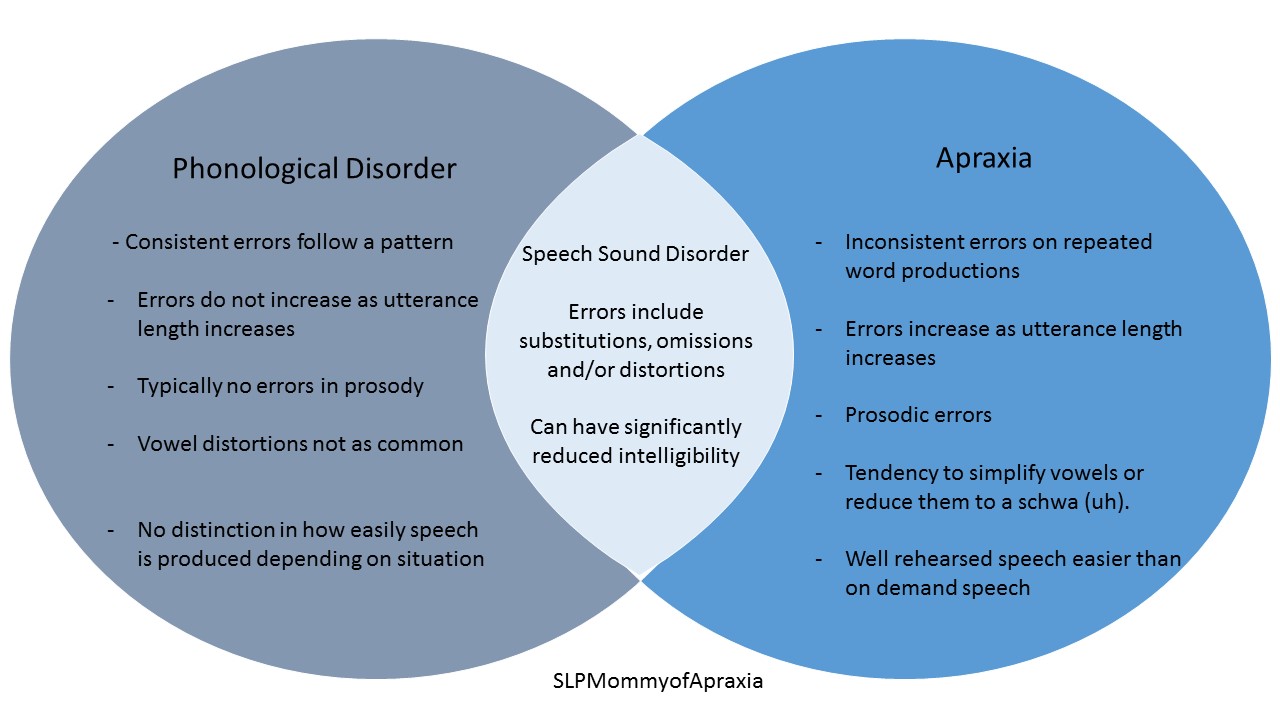
Graphic depicting the differences and overlap between phonological disorder and apraxia.
Language delays do not involve the actual production of speech sounds (although the two can overlap). Language delays can be caused by many factors as well, and include:
1.) A late talker – A late talker is just a typical child who talks late and has no additional speech or language issues from it. The ASHA website offers this explanation “At onset, it is difficult to distinguish late talkers from late bloomers, as this distinction can be made only after the fact,” which as a parent and professional of children with apraxia, this is a pretty DANGEROUS and potentially hazardous distinction if you are just waiting around to see if it’s late blooming or something else.
2.) A language impairment – There are many components of language. Language is comprised of five major components including: phonology, morphology, semantics, syntax, and pragmatics. In addition, children can have difficulties expressively or receptively with these components. Some children can have both, getting a diagnosis of MERLD or mixed expressive/receptive language disorder.
3.) A hearing loss – This is repeated on this list, because a hearing loss can also cause delays in language development as well. ASHA describes its effects in the following:
There are four major ways in which hearing loss affects children:
- It causes delay in the development of receptive and expressive communication skills (speech and language).
- The language deficit causes learning problems that result in reduced academic achievement.
- Communication difficulties often lead to social isolation and poor self-concept.
- It may have an impact on vocational choices.
3.) A medical or genetic condition – Other causes of language delay or impairment could be but aren’t limited to:
Autism
Fragile X
Down Syndrome
Cerebral Palsy
Cleft lip/palate
To complicate things even more, a child with a medical disorder could also have a co-morbid speech or language impairment as well! It’s important to always know the etiology because an accurate diagnosis ensures and informs therapy.
What I hoped to clarify in this post is that the question “Does this look like apraxia?” is just a little (okay a lot) more complicated than it seems. Obviously the best place to start is to get a comprehensive evaluation! If apraxia is suspected, it is best to get a differential diagnosis from an SLP who has received additional training past their post graduate degree in apraxia of speech.
To find an apraxia expert near you, or to get listed as an apraxia expert, go to apraxia-kids.org and click “find a speech therapist” at the top.